Depression as a Comorbidity to Diabetes: Implications for Management
Andrea A. Riley; Mindy L. McEntee; Linda Gerson; Cheryl R. Dennison
Published: 09/25/2009
Abstract and Introduction
Abstract
Research has established a link between depression and diabetes, even though the underlying mechanisms in this relationship remain unclear. Primary care providers are often responsible for managing these conditions and are well positioned to provide integrated care improving patients' physical and mental health outcomes, yet they face a number of barriers contributing to the inadequate management of depression in primary care. All diabetic patients should be routinely screened for depression; management of these concomitant conditions should use a comprehensive approach that may include medication or referral for psychotherapy. This paper explores the relationship between depression and diabetes and implications for practice in the areas of screening, diagnosis, and management of depression in diabetic patients.
Introduction
The odds of having depression among individuals with type 1 or 2 diabetes are more than twice that of non-diabetics, [1] with an estimated 33% of diabetics experiencing depressive symptoms severe enough to warrant treatment at any single point in time. [2] The course of depression in these individuals is often chronic [3] and may adversely affect the course of coexisting medical conditions. [4–6] A number of studies have found depression to be associated with poor self-care in people with diabetes. [7–13] Decreased adherence to medication, [7,10,13–15] diet, [7,8,13,14] exercise, [8,11,13] and blood glucose monitoring [13] may contribute to increased diabetic symptoms, [8,16] glucose dysregulation, [17–19] diabetic complications, [18,20,21] mortality, [22–24] decreased physical [7,8,25] and mental functioning, [7,26] lower quality of life, [7,27] and increased healthcare utilization [7,26,28] associated with comorbid diabetes and depression.
Because primary care providers (PCPs) are frequently charged with the management of type 2 diabetes and uncomplicated unipolar depression, they are well positioned to provide integrated care for these concomitant disorders. [29] While the co-occurrence of these conditions is a widely known clinical phenomenon, depression remains under-recognized and inadequately treated in primary care. [2,13,29–32] To provide high-quality care optimizing physical and mental health outcomes for their patients, it is important that PCPs understand the relationship between depression and diabetes. This paper examines the etiologies of these comorbid conditions and discusses implications for practice in the areas of screening, diagnosis, and management of depression in the diabetic population.
Relationship between Diabetes and Depression
The high prevalence of comorbid depression and diabetes suggests that these disorders may be related. [33] Depression has been proposed as both a result of and precursor to diabetes, with this relationship attributed to a variety of mechanisms. Studies have examined a number of psychosocial and biological correlates of depression and diabetes, yet the causal relationship between these disorders, its direction, and underlying mechanisms remain unclear. [31,34]
Depression as a Result of Diabetes
Some authors have proposed that depression may stem from the psychosocial burden and/or biochemical changes related to diabetes and its treatment. [1,17,18] This hypothesis may help explain why depression is more prevalent in diabetics than in the general population and is supported by the temporal finding among type 1 diabetics, in which diabetes typically precedes the onset of major depressive disorder (MDD). [34] While there is little empirical data on the psychosocial facet of this theory, there is some evidence that emotional distress is mediated by perceived threat of illness, [35,36] self-esteem, [37,38] self-efficacy, [35] coping skills, [39] and social support. [35,37]
Sociodemographic factors including younger age, [21,26,40] female gender, [1,21,26,40–44] low socioeconomic status, [26,43,45] ethnic minority status, [21,31,41,46] chronic stressors, and negative life events [47] have also been identified as predictors of depression among individuals with diabetes, although a causal relationship has not been established.
The biological component of this hypothesis speculates that the metabolic consequences of diabetes lead to structural and functional changes in the brain that increase susceptibility to stress and depression, [48] although data thus far have been inconclusive. The relationship between depression and glycemic control remains subject to debate; a meta-analysis of 26 studies found a significant relationship with comparable effect sizes in both type 1 and type 2 diabetes, [17] yet other research did not find this correlation, [42,49,50] or found it significant only for individuals with type 1 diabetes. [51,52] The connection between diabetic complications and depression has also produced mixed results; [18,31,44,53–57] these discrepancies may suggest that biochemical mechanisms have greater influence on the duration of depression rather than its initial onset. [34]
Depression as a Precursor to Diabetes
An alternative hypothesis in which depression precedes and predisposes individuals to diabetes may explain the development of type 2 diabetes among patients diagnosed with depression several years earlier. [58] This theory proposes that diabetes may develop via the psychosocial effects of depression, including adiposity and negative health behaviors like poor diet, physical activity, smoking, and medication adherence; and/or as a result of biological mechanisms such as activation of the HPA axis [45,59–62] and inflammatory responses [63–66] that contribute to insulin resistance and decreased glucose uptake. A meta-analysis of 9 longitudinal studies showed that adults who were depressed were 37% more likely to develop type 2 diabetes than their non-depressed counterparts. [67] Other studies have shown that this increased risk remains significant after controlling for known demographic and clinical risk factors. [57,68–75] Adults receiving treatment for depression were still prone to developing diabetes, [75,76] with those taking a tricyclic antidepressant (TCA) and a selective serotonin reuptake inhibitor (SSRI) concurrently at greater risk (60%) than those prescribed either a TCA (44%) or SSRI (37%) alone. [77]
While research supports a trend in which depression precedes type 2 diabetes, causal mechanisms for this association remain speculative. A recent meta-analysis of 13 prospective studies found that while adverse psychosocial factors were associated with poor diabetes control in both type 1 and type 2 diabetes, they were not related to incidence of diabetes. [78] Variations in the extent to which depression increased the risk of type 2 diabetes after accounting for known risk factors suggest that additional factors affect this relationship. [44,57,70] Inflammatory markers interleukin-6 and C-reactive protein were elevated in depressed individuals and have been identified as risk factors for developing type 2 diabetes, yet models accounting for these variables were still unable to explain the association between depression and the incidence of type 2 diabetes in Golden et al. [44] Knol et al found that insulin resistance was not related to depressive symptoms, further challenging the proposed mechanisms underlying this relationship. [79]
A Bidirectional Relationship
Contradictory research findings suggest the relationship between depression and diabetes is complex and may differ for type 1 and type 2 diabetes. The factors underlying this relationship may be bidirectional and consist of multiple mechanisms and/or indirect causation. Golden et al found evidence for a bidirectional relationship within the same cohort; adults with treated type 2 diabetes who were depression-free at baseline were 52% more likely to experience depressive symptoms than non-diabetics, while adults with elevated depression scores were 21% more likely than those with low or normal symptoms to develop type 2 diabetes after adjusting for clinical, demographic, and lifestyle risk factors. [44]
Screening and Diagnosis
Although the link between depression and diabetes remains elusive, adverse effects can be minimized by adequate recognition and treatment. Because both conditions can produce similar somatic symptoms, concern has been raised that current diagnostic criteria for depression are not appropriate for the diabetic population. [80] While rates of sympathetic arousal, gastrointestinal complaints, and fatigue are higher in depressed individuals with co-occurring medical conditions, the differences are modest and did not significantly affect the diagnostic process. [81,82] Depressed diabetics experienced a similar course of depression and were just as likely to respond to treatment as depressed individuals without diabetes, even though they reported lower levels of somatic well-being and contentment. [83] Moreover, mean scores and symptom profiles on the Beck Depression Inventory (BDI) did not significantly differ between depressed individuals with diabetes and those without. [80] These findings suggest that diagnostic criteria and screening methods currently accepted for use in the general population are also suitable for diabetic patients.
Current research suggests only 25% to 50% of diabetic patients with depression are identified in primary care. [32,84,85] The American Diabetes Association (2008) advises regular screening throughout the course of diabetes management: at diagnosis, routine management visits, hospitalizations, when complications develop, or when problems with glucose control, quality of life, or adherence to self-care are identified. [86] Administration of a brief depression screening tool should be included with annual screening for diabetes-related parameters.
Selectively screening individuals based on the presence of known risk factors alone is not recommended, as presence of these factors is not as reliable as use of brief screening tools in detecting depression. [87] Providers should, however, be mindful of certain triggers in patients' medical history that may warrant additional screening, including unexplained psychosomatic symptoms, history of depression, comorbid psychological illnesses, chronic pain, substance abuse, [87] or reported diabetes symptoms disproportionately high with respect to the course of diabetes. [16] Patients with a personal history of depression or current anxiety disorder are significantly more likely to have depression and may warrant a diagnostic interview instead of initial screening. [87]
Depression Screening Tools
While guidelines agree routine screening for depression is necessary, they provide little guidance on selecting the best measure(s) to do so. [86,87] Several self-report questionnaires have been validated to assess depressive symptoms in primary care patients, although their use in diabetic populations has received considerably less study. Nevertheless, several screening tools have demonstrated sound psychometric properties detecting depression in samples of primary care patients with diabetes ( Table 1 ). In spite of differences in length, wording, and scoring criteria, each of these measures can be completed and scored within 5 to 10 minutes, allowing providers to follow up on the results of screening during the same visit.
Table 1. Depression Screening Tools for Use in Primary Care
Screening Tool
Public Domain
No. of Items
Time to Administer
Score Range
Usual Cut-point
Reliability & Validity in Primary Care Patients
Reliability & Validity in Diabetic Patients
Beck Depression Inventory II (BDI-II)
No
21
2–5 minutes
0–63
14–19 = Mild
20–28 = Moderate
29–63 = SevereArnau 2001 – cutoff 18
Sensitivity 94%
Specificity 92%
AUC = 0.96Lustman 1997** – cutoff 13
Sensitivity 85%
Specificity 88%
AUC 0.94Beck et al 1996
Dutton 2004 – cutoff 14
Cronbach α = 0.90
Sensitivity 88%
Specificity 84%
AUC = 0.91**only original BDI validated in this population
Beck Depression Inventory for Primary Care (BDI-PC)
No
7
<2 minutes
0–21
≥4
Steer 1999 – cutoff 4
Cronbach α = 0.85
Sensitivity 97%
Specificity 99%
AUC = 0.99n/a
Beck et al 1997
Beck 1997 outpatient – cutoff 6
Cronbach α = 0.88
Sensitivity 83%
Specificity 95%
Center for Epidemiological Studies Depression Scale (CES-D)
Yes
20
2–5 minutes
0–60
≥16
Whooley 1997 – cutoff 16
Sensitivity 88%
Specificity 74%
AUC = 0.89Hermanns 2006 – cutoff 14
Sensitivity 79%
Specificity 89%
AUC = 0.80Radloff et al 1977
McHale 2000 – cutoff 16
Sensitivity 71%
Specificity 71%
AUC = 0.81
Zauszniewski 2008 cutoff 16
Cronbach α = 0.87Patient Health Questionnaire – 9 (PHQ-9)
Yes
9
<2 minutes
0–27
5–9 = Mild
10–14 = Moderate
≥15 = SevereKroenke 2001 – cutoff ≥ 10
Cronbach α = 0.89
Sensitivity 88%
Specificity 88%
AUC = 0.95Kahn 2008 – cutoff ≥ 10
Sensitivity 66%
Specificity 52%Kroenke 2001
Lowe 2002 – cutoff ≥10
Cronbach α = 0.88
Sensitivity 81%
Specificity 82%
AUC = 0.95Lamers 2008 – cutoff ≥7
Sensitivity 92%
Specificity 81%Patient Health Questionnaire – 2 (PHQ-2)
Yes
2
<1 minute
0–6
≥3
Kroenke 2003 – cutoff ≥3
Sensitivity 83%
Specificity 92%
AUC = 0.93Daly 2007 – cutoff ≥3
Sensitivity 83%
Specificity 92%Kroenke 2003
Brody 1998 – cutoff ≥ 3
Sensitivity 65%
Specificity 99%
WHO-Five Well-being Index (WHO-5)
Yes
5
<2 minutes
0–25
<13
Henkel 2004 – cutoff <13
Sensitivity 94%
Specificity 63%
AUC = 0.91De Wit 2007 – cutoff <13
Cronbach α = 0.82
Sensitivity 89%
Specificity 86%World Health Organization 1998
Lowe 2002 – cutoff <13
Cronbach α = 0.91
Sensitivity 94%
Specificity 78%
AUC = 0.91Awata 2007 – cutoff <13
Cronbach α = 0.89
Sensitivity 100%
Specificity 78%
AUC = 0.92Zung Self-Rating Depression Scale (SDS)
Yes
20
2–5 minutes
0–100
50–59 = Mild
60–69 = Moderate
≥70 = SevereOkimoto 1982 – cutoff ≥ 60
Sensitivity 82%
Specificity 87%Rajala 1997 – cutoff > 55
Sensitivity 72%
Specificity 83%Reliability and validity data for these instruments is also summarized in Table 1 . Cutoff scores optimizing the sensitivity and specificity of these measures were determined through receiving operator characteristics (ROC) analysis, while area under the ROC curve (area under the curve [AUC] index) assessed how well an instrument could discriminate between depressed and nondepressed individuals. Small variations in these statistics were reported across studies, though overall there was little difference between primary care (sensitivity 81–97%, specificity 63–99%, AUC 0.89–0.95) and diabetic patients (sensitivity 66–100%, specificity 52–92%, AUC 0.80–0.94). Because there is little evidence to suggest that any one of these measures is superior to the others, PCPs may wish to use the 2-item Patient Health Questionnaire (PHQ-2) as an initial screening tool for diabetic patients ( Table 2 ). For those who indicate they have been bothered in the last 2 weeks from either "little interest or pleasure in doing things" or "feeling down, depressed, or hopeless," providers can investigate further by administering the 9-item Patient Health Questionnaire-9 (PHQ-9) ( Table 3 ). This combination of tools, available in public domain, provides an effective method of screening for depression that also addresses time constraints frequently encountered by PCPs.
Table 1. Depression Screening Tools for Use in Primary Care
Screening Tool
Public Domain
No. of Items
Time to Administer
Score Range
Usual Cut-point
Reliability & Validity in Primary Care Patients
Reliability & Validity in Diabetic Patients
Beck Depression Inventory II (BDI-II)
No
21
2–5 minutes
0–63
14–19 = Mild
20–28 = Moderate
29–63 = SevereArnau 2001 – cutoff 18
Sensitivity 94%
Specificity 92%
AUC = 0.96Lustman 1997** – cutoff 13
Sensitivity 85%
Specificity 88%
AUC 0.94Beck et al 1996
Dutton 2004 – cutoff 14
Cronbach α = 0.90
Sensitivity 88%
Specificity 84%
AUC = 0.91**only original BDI validated in this population
Beck Depression Inventory for Primary Care (BDI-PC)
No
7
<2 minutes
0–21
≥4
Steer 1999 – cutoff 4
Cronbach α = 0.85
Sensitivity 97%
Specificity 99%
AUC = 0.99n/a
Beck et al 1997
Beck 1997 outpatient – cutoff 6
Cronbach α = 0.88
Sensitivity 83%
Specificity 95%
Center for Epidemiological Studies Depression Scale (CES-D)
Yes
20
2–5 minutes
0–60
≥16
Whooley 1997 – cutoff 16
Sensitivity 88%
Specificity 74%
AUC = 0.89Hermanns 2006 – cutoff 14
Sensitivity 79%
Specificity 89%
AUC = 0.80Radloff et al 1977
McHale 2000 – cutoff 16
Sensitivity 71%
Specificity 71%
AUC = 0.81
Zauszniewski 2008 cutoff 16
Cronbach α = 0.87Patient Health Questionnaire – 9 (PHQ-9)
Yes
9
<2 minutes
0–27
5–9 = Mild
10–14 = Moderate
≥15 = SevereKroenke 2001 – cutoff ≥ 10
Cronbach α = 0.89
Sensitivity 88%
Specificity 88%
AUC = 0.95Kahn 2008 – cutoff ≥ 10
Sensitivity 66%
Specificity 52%Kroenke 2001
Lowe 2002 – cutoff ≥10
Cronbach α = 0.88
Sensitivity 81%
Specificity 82%
AUC = 0.95Lamers 2008 – cutoff ≥7
Sensitivity 92%
Specificity 81%Patient Health Questionnaire – 2 (PHQ-2)
Yes
2
<1 minute
0–6
≥3
Kroenke 2003 – cutoff ≥3
Sensitivity 83%
Specificity 92%
AUC = 0.93Daly 2007 – cutoff ≥3
Sensitivity 83%
Specificity 92%Kroenke 2003
Brody 1998 – cutoff ≥ 3
Sensitivity 65%
Specificity 99%
WHO-Five Well-being Index (WHO-5)
Yes
5
<2 minutes
0–25
<13
Henkel 2004 – cutoff <13
Sensitivity 94%
Specificity 63%
AUC = 0.91De Wit 2007 – cutoff <13
Cronbach α = 0.82
Sensitivity 89%
Specificity 86%World Health Organization 1998
Lowe 2002 – cutoff <13
Cronbach α = 0.91
Sensitivity 94%
Specificity 78%
AUC = 0.91Awata 2007 – cutoff <13
Cronbach α = 0.89
Sensitivity 100%
Specificity 78%
AUC = 0.92Zung Self-Rating Depression Scale (SDS)
Yes
20
2–5 minutes
0–100
50–59 = Mild
60–69 = Moderate
≥70 = SevereOkimoto 1982 – cutoff ≥ 60
Sensitivity 82%
Specificity 87%Rajala 1997 – cutoff > 55
Sensitivity 72%
Specificity 83%Table 2. Patient Health Questionnaire-2 (PHQ-2)
Over The Past 2 Weeks, How Often Have You Been Bothered By Any Of The Following Problems?
Not At All
Several Days
More Than Half The Days
Nearly Every Day
Little interest or pleasure in doing things
0
1
2
3
Feeling down, depressed, or hopeless
0
1
2
3
Developed by Drs. Robert L. Spitzer, Janet B.W. Williams, and Kurt Kroenke and colleagues, with an educational grant from Pfizer Inc. For research information, contact Dr. Spitzer at rls8@columbia.edu.
Copyright © 2005 Pfizer, Inc. All rights reserved. Reproduced with permission.Table 3. Patient Health Questionnaire-9 (PHQ-9)
Over The Last 2 Weeks, How Often Have You Been Bothered By Any Of The Following Problems?
Not At All
Several Days
More Than Half The Days
Nearly Every Day
1. Little interest or pleasure in doing things
0
1
2
3
2. Feeling down, depressed, or hopeless
0
1
2
3
3. Trouble falling or staying asleep, or sleeping too much
0
1
2
3
4. Feeling tired or having little energy
0
1
2
3
5. Poor appetite or overeating
0
1
2
3
6. Feeling bad about yourself- or that you are a failure or have let yourself or your family down
0
1
2
3
7. Trouble concentrating on things, such as reading the newspaper or watching television
0
1
2
3
8. Moving or speaking so slowly that other people could have noticed? Or the opposite — being so fidgety or restless that you have been moving around a lot more than usual
0
1
2
3
9. Thoughts that you would be better off dead or of hurting yourself in some way
0
1
2
3
Office coding: Total Score _____________ =
0
+
____
+
____
+
____
If you checked off any problems, how difficult have these problems made it for you to do your work, take care of things at home, or get along with other people?
Not difficult at all
Somewhat difficult
Very difficult
Extremely difficult
Developed by Drs. Robert L. Spitzer, Janet B.W. Williams, and Kurt Kroenke and colleagues, with an educational grant from Pfizer Inc.
Copyright © 2005 Pfizer, Inc. All rights reserved. Reproduced with permission.Management of Depression in Diabetes
To optimize patient outcomes, PCPs should have a thorough understanding of research findings related to the treatment of depression in diabetes. While necessary, provider education and screening alone had little impact on patient outcomes and other barriers to management. [14,87,88] Depression remains inadequately treated in primary care, [2,13,31,89] with patients receiving inappropriately titrated doses of antidepressants [90] and up to 50% discontinuing use prior to achieving remission. [91] Both psychopharmacology [92–101] and psychotherapy [102–107] have been shown to effectively treat depression in diabetic patients, yet studies estimate only 33% to 52% of these patients were prescribed antidepressants, [2,32,108] while less than 20% completed 4 or more counseling sessions. [32]
Antidepressants are the most common pharmacological treatment option, although PCPs class selection must take into account a patient's presenting symptoms, comorbid medical conditions, drug interactions, and side effects. Because most antidepressants have little impact on the course of depression once discontinued and relapse following successful treatment is common, [89] a comprehensive treatment approach by the PCP should consider a referral for psychotherapy in addition to initial treatment and maintenance with medication. Both psychotherapy and medications are effective treating depression in diabetics, although the combination of these approaches has been shown to be more effective than either treatment alone in nondiabetic samples. [109] Monoamine oxidase inhibitors (MAOIs) are not recommended in diabetic patients due to associated dietary restrictions, weight gain, and the potential for sudden, severe hypoglycemia. [97,99] Research findings and considerations for the use of TCAs, SSRIs, newer antidepressants, and cognitive behavior therapy (CBT) are summarized below.
Tricyclic Antidepressants
TCAs are the oldest class of antidepressants and were commonly prescribed in primary care before the development of safer alternatives like SSRIs. Serious risks associated with the use of TCAs limit their current use, most notably due to cardiac effects [92,110–112] and lethality in overdose. [113] Weight gain, [92,97,110,114] hyperglycemia, [92,97] anticholinergic effects, [110] and impaired memory [97] also contribute to the limited use of these medications in patients with diabetes. In spite of their side effects, TCAs may aid in regulating sleep [110,112] and are well established as a treatment for diabetic neuropathy; both desipramine and amitriptyline were shown to be more effective treating neuropathy than the SSRI fluoxetine in a randomized, double-blind, placebo-controlled study. [115] While the TCA nortriptyline effectively reduced depressive symptoms among diabetics in a double-blind, placebo-controlled trial, it produced an adverse hyperglycemic effect unrelated to the drug's effect on weight. A similar increase in fasting blood glucose was found in nondiabetic patients following treatment with imipramine, [116] adding to the concern of TCAs in individuals with diabetes. Consequently, TCAs are not recommended as a first-line treatment for this population, and should only be considered when patients are unresponsive to trials of at least 2 newer antidepressants.
Selective Serotonin Reuptake Inhibitors
SSRIs are frequently a first-line choice of antidepressants in primary care, treating depression as effectively as TCAs with fewer adverse effects. [112,117,118] SSRIs have received a significant amount of study in diabetic patients, examining the effect of these drugs on depression as well as diabetes outcomes and self-care. Fluoxetine, [93,100,116] sertraline, [95,98,119] and paroxetine [100,101,120] were all effective treating depression in this population; fluoxetine and paroxetine were also associated with improved quality of life. [100] There was little evidence for superior effectiveness of one SSRI over another in any study, although patients treated with fluoxetine experienced a reduction in depression severity 2 weeks earlier than those receiving paroxetine. [100] Fluoxetine has also been associated with moderate weight loss, [121] though the effect of other SSRIs on weight has been inconsistent. [114] While SSRIs are associated with substantially fewer anticholinergic and cardiovascular effects, side effects such as sexual dysfunction, gastrointestinal distress, and agitation remain fairly common in diabetics and should be taken into consideration. [110]
Several randomized controlled trials have demonstrated a trend toward improvement in HgbA1c levels with SSRI treatment, [93,95,100,120] with statistically significant change in 2 open-label studies. [95,98] Musselman et al noted that the metabolic effect of SSRIs on certain oral antihyperglycemic agents may increase the risk of hypoglycemia, yet no clinical interaction of these drugs have been reported. [68] While the majority of treatment studies ranged from 8 to 12 weeks, a year-long maintenance regimen of sertraline following successful treatment found patients taking the drug were less likely to experience recurring depression than those receiving placebo. [95] Moreover, the initial improvement in glycemic control during treatment was sustained throughout the maintenance phase. [95] Based on this research, PCPs can prescribe an SSRI to treat depression with reasonable confidence that the medication will not worsen the course of diabetes and may even contribute to better glycemic control.
Research examining the use of SSRIs in the treatment of diabetic neuropathy is limited. Randomized, double-blind, placebo-controlled trials have demonstrated the effectiveness of paroxetine [122] and citalopram, [123] although a number needed to treat analysis suggests they were less effective than TCAs. [124] Two 8-week open trials found sertraline improved neuropathic symptoms, yet its effectiveness has not been compared to other treatments. [125] Fluoxetine was the only SSRI studied in the treatment of depressed patients with neuropathy; although the drug was associated with improved neuropathic symptoms, its effects were no different than placebo. [115] Thus, while SSRIs are better tolerated than TCAs and have been well established to effectively treat depression, they are not deemed a sufficient choice for neuropathy. [126]
Newer Antidepressants
Several other new antidepressants are widespread in use, including serotonin-norepinephrine reuptake inhibitors (SNRIs), norepinephrine-dopamine reuptake inhibitors (NDRIs), and noradrenergic and specific serotonergic antidepressants (NASSAs). Like SSRIs, antidepressants in these classes are generally considered safer alternatives to TCAs for the treatment of depression. Many of these newer drugs may have indications for use either as a first-line treatment or when patients do not respond to SSRIs, although research on their use in diabetic patients is extremely limited.
SNRIs have been shown to effectively treat diabetic neuropathy in addition to depression. Duloxetine was approved by the FDA for this purpose in 2004 and is generally well-tolerated, with fewer adverse events than routine care. [127,128] While associated with a modest increase in fasting glucose and A1C, long-term studies have found no adverse effects of duloxetine on lipid profiles or weight. [127–129] The relative efficacy of another SNRI, venlafaxine, was comparable to TCAs and gabapentin for the treatment of neuropathy, [130] although this drug was associated with higher rates of adverse serotonergic effects and dose-dependent hypertension than duloxetine. [131]
Other side effects are similar to SSRIs and remain more conducive to use in diabetic patients than TCAs, [132] although these drugs should not be abruptly discontinued due to risk of serious withdrawal symptoms. These findings suggest that SNRIs may be a viable treatment option for depressed patients with diabetic neuropathy, although these drugs have yet to be studied in patients with comorbid diabetes and depression.
The NDRI bupropion is the only newer antidepressant to be studied in diabetic patients with depression. Unlike SSRIs, bupropion effectively treated depression without sexual side effects [96,133] or concern of altering the metabolism of oral hypoglycemic medications, [68] although increased anxiety, nausea, dizziness, and skin irritation were reported. Implications for long-term use of bupropion were promising: patients who stayed on maintenance treatment of the drug had no recurring depression. [96] Bupropion has also been shown to be useful for smoking cessation in diabetics and has minimal impact on weight, ranging from no change to modest loss. [96,133] Only one study has examined the effects of this NDRI on neuropathy, although the drug was more effective than placebo with nearly 70% of patients reporting improvement. [134] Like SNRIs, the NDRI bupropion may be an alternative to SSRIs in diabetic patients with neuropathy, although it should be noted that this is the only antidepressant not effective in relieving symptoms of anxiety. [135]
The NASSA mirtazapine has received the least study in the diabetic population. A randomized double-blind trial found mirtazapine relieved depressive symptoms significantly earlier than fluoxetine and was equally tolerable without sexual side effects or other adverse events related to serotonin. [136] Commonly reported side effects of somnolence, hyperphagia, and weight gain have led to some concern using mirtazapine in patients with diabetes; although patients taking the drug have experienced significant weight gain, glycemic control actually improved. [137,138] While no research to date has examined the use of mirtazapine in diabetic neuropathy, the drug has been shown to increase pain tolerance in healthy individuals [139] and provide significant relief to depressed patients with chronic pain. [140]
Cognitive Behavior Therapy
Several studies have shown CBT and its variants to be successful in relieving symptoms of depression in diabetics. [102–106,141] Unlike antidepressants, there is evidence that the beneficial effects of CBT are maintained for up to a year past the end of treatment. [103,105] Therapy has also been shown to improve patients' self-efficacy [104] and diabetes management, [102] while glycemic control improved in some [102,105,106,141] but not all [103–105,141] studies. Psychotherapeutic approaches are beneficial in that they lack the side effects of medication, but require active patient participation and may not be well received in all patients. Poor integration with specialty mental health care and the stigma associated with mental illness are also barriers to this form of treatment. [29,89] Providers should discuss the option of psychotherapy with depressed diabetic patients as a part of a comprehensive treatment plan, but be aware of potential barriers to this course of treatment.
Implications for the PCP
Research supports a clear association between diabetes and depression, even though the mechanisms underlying this relationship are not well understood. PCPs are frequently responsible and well positioned to manage these comorbid disorders and are advised to proactively screen for, diagnose, and treat depression to optimize patient outcomes, yet a number of barriers contribute to depression being inadequately managed in primary care. Suboptimal recognition can be addressed by increasing provider knowledge and following current treatment guidelines for routine depression screening of all diabetic patients, whether or not known risk factors for depression are present. Several screening tools have been validated in diabetic patients that can be completed in less than 10 minutes; use of the PHQ-2 to determine whether further investigation with PHQ-9 is warranted may help optimize the efficiency of the screening process. Providers should also be aware that presenting symptoms of depression can differ and should be sensitive to patients' gender, race, ethnicity, and individual values and beliefs. [2,108,142]
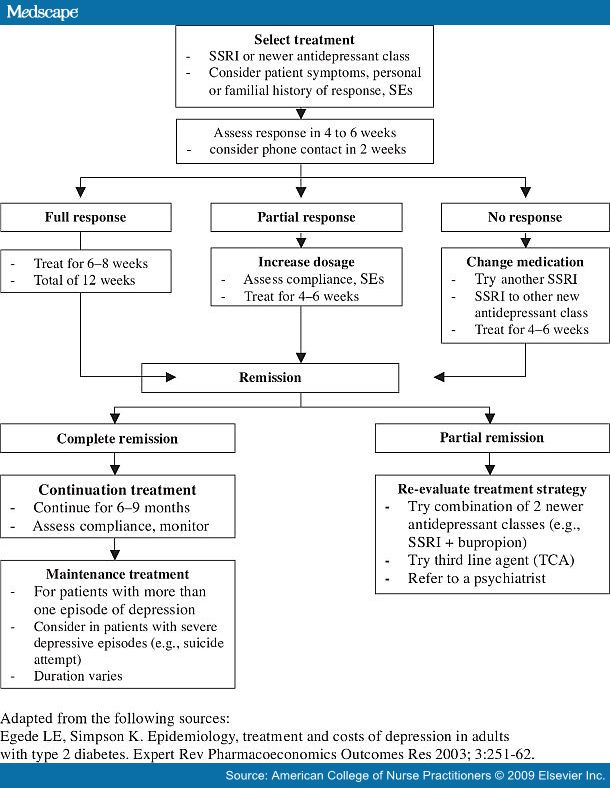
Management of depression in diabetes should be approached in a comprehensive manner, which potentially includes both medication and referral for psychotherapy such as CBT. Patients resistant to treatment should be educated to understand that benefits extend beyond improved mood and may include pain relief; decreased anxiety; improved social, occupational, and physical activity; enhanced general and sexual functioning; decreased preoccupation with somatic symptoms; more normal sleep and eating habits; improved coping skills; and better diabetes care. [2,94] Other patient barriers can be circumvented by selecting a treatment(s) that match an individual's symptoms, taking his or her preferences into consideration, [2] and including patients' partners or other key family members whenever possible. [112] Management barriers imposed at the system level include time constraints limiting close follow-up and monitoring, competing clinical priorities, and poor integration with mental health care. Treatment studies have demonstrated a clear need for PCPs to have additional mental health support, [12] which may relieve some of the burden experienced by providers in primary care. Treatment algorithms for pharmacological treatment of depression in primary care patients with diabetes provide further assistance for PCPs clinical decisions. [31,89] Concordant with the research summarized here, these guidelines recommend initial treatment with an SSRI or other new antidepressant, taking into account patients' personal or familial responses to specific medications, in addition to side effects. [31,89] The timeline and further indications for follow-up assessment based on these recommendations are listed in Figure 1.
Figure 1. Antidepressant treatment algorithm for primary care patients with diabetes
PCPs are also likely to be aided by future research addressing gaps in the current body of literature. Much of the research on comorbid depression in diabetic patients is limited to MDD; treatment for subclinical or other depressive disorders has received little study, even though these conditions may produce similar effects to MDD. Trials of newer antidepressants are promising, although there is little research on their use in the diabetic population. Antidepressant maintenance therapy has been identified as necessary, yet the long-term outcomes associated with it are unknown. Moreover, there is a need for collaborative care programs to identify effective and efficient ways to integrate treatment for these conditions in primary care.
Conclusion
Family and adult NPs and other PCPs can optimize health outcomes by increasing their understanding of the relationship between depression and diabetes and by systematically screening for, diagnosing, and managing depression in diabetic patients. While research in the area is limited, appropriate screening strategies have been identified and benefits and risks of certain pharmacological and psychotherapeutic treatments have been shown. Findings presented in this paper should serve as a guide in clinical decision making for the diagnosis and treatment of primary care patients with comorbid depression and diabetes.
-See: Journal for Nurse Practitioners. 2009;5(7):523-535 or http://www.medscape.com/viewarticle/708407 for full references.
10/09