The Experience of Partners in a
Sexual Relationship With a Person With Cancer
Abstract
Changes in sexuality and intimacy after cancer were examined using open-ended questionnaire responses with 156 informal carers who were partners of a person with cancer. Interviews were conducted with 20 participants to examine changes in depth. Seventy-six percent of partners of a person with "nonreproductive" cancer types and 84% of partners caring for a person with cancer involving "reproductive" sites reported an impact on their sexual relationship. Cessation or decreased frequency of sex and intimacy was reported by 59% of the women and 79% of the men. Renegotiation of sexuality and intimacy after cancer was reported by only 19% of the women and 14% of the men. Reasons for changes to sexuality after cancer were the impact of cancer treatments, exhaustion due to caring, and repositioning of the person with cancer as a patient, not a sexual partner. Changes to sexuality were associated with reports of self-blame, rejection, sadness, anger, and lack of sexual fulfillment. Positive consequences of changes included accepting the changed sexual relationship and having increased closeness and intimacy. These findings reinforce the need to acknowledge the sexual needs of partners as well as people with cancer, by healthcare professionals working in cancer and palliative care.
Introduction
It is now widely recognized that cancer and its treatment can have a significant effect on the quality of life of both people with cancer and family members providing informal care, particularly their intimate partner. [1] Sexuality and intimacy are important aspects of quality of life, [2] and there is a growing body of evidence to show that cancer can result in dramatic changes to sexuality, sexual functioning, relationships, and sense of self. [3-5] These changes can be experienced as the most significant in the life of a person with cancer [6] and can lead to emotional distance between couples, [7] as well as feelings of isolation, anxiety, depression, [8] or inadequacy. [9]
Whereas the experiences of partners are often neglected in research on sexuality and intimacy after cancer, [10] there is growing acknowledgment of their unmet needs in this area. [11,12] Reported disruptions include decreases in their own sex drive, fear of initiating sex with their partner, difficulty regaining a level of "normality" within the sexual relationship, and feeling unwanted and unattractive because of cessation of sex. [4,13,14] It has also been argued that when sexual intercourse ceases in the context of illness, touching and other forms of affectionate physical contact also diminish [15] because of a perception among some couples that these forms of affection necessarily lead to sexual intercourse, which is either not possible or deemed inappropriate. [16]
One of the limitations of research in this area is the focus on experiences of sexuality after cancer that affects the reproductive organs. [4,13,14] There is a need for research examining the experiences of partners across a range of cancer types, as cancers that do not involve parts of the body designated as "sexual" or "reproductive" may also impact on sexuality. [10] A further related limitation is the focus on the physiological effects of cancer and its treatment upon the sexuality of partners. However, the dynamics of the caregiving relationship and social constructions surrounding what constitutes appropriate sexual conduct after cancer may also interfere with a couples' sexual relationship. For example, partners who provide a great deal of intimate physical care to the person with cancer (such as helping with toileting or feeding) can experience difficulties in continuing to see them as a sexual person [17] and reposition them as a "patient" [18] or as asexual. [19] Broader cultural constructions of normative sexuality may also be influential in determining the ability of couples to renegotiate sexuality and intimacy after cancer, particularly when sexual intercourse is no longer possible. As Judith Butler [20] has argued, our understanding of sexual subjectivity is confined within a "heterosexual matrix," within which masculinity and femininity are performed through engagement in normative sexual practices described as the "coital imperative," [21] with failure to perform coitus positioned as "dysfunction" and other practices referred to as not "real sex." [22] This provides a theoretical framework for understanding why many heterosexual couples who cannot physiologically engage in sexual intercourse after diagnosis and treatment of cancer cease all expression of sexual intimacy. It also suggests that the dynamics and pressures of the caring role, as well as constructions and beliefs about what is acceptable or appropriate sexually after cancer, are worthy of investigation.
The aim of the present study was to examine the subjective experience of sexuality and intimacy after the diagnosis and treatment of cancer for partners of a person with cancer across a range of cancer types using qualitative methods within a critical realist epistemological standpoint. Advocated as the way forward for research examining health in a sociocultural context, [23] critical realism recognizes the materiality of the body and other aspects of experience (such as cancer, cancer treatments, the caring role) but conceptualizes this materiality as always mediated by culture, language, and subjectivity. [24] A variety of methodological approaches, both qualitative and quantitative, are valued equally within a critical realist approach, and there is acceptance of the legitimacy of subjective experience, often marginalized in mainstream health psychology research.
Methods
Participants and Recruitment
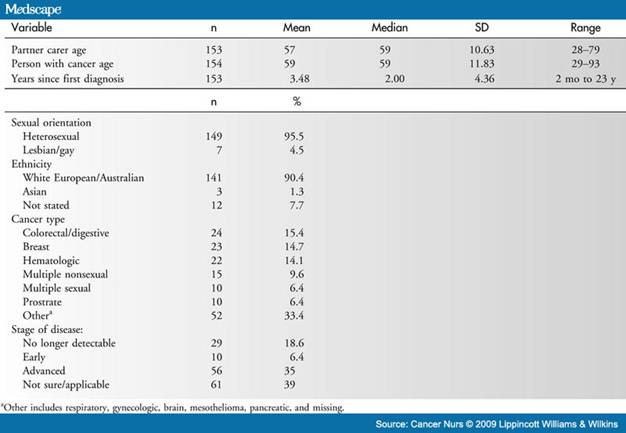
One hundred fifty-six informal carers (55 men, 101 women) were selected from their participation in a larger mixed-methods study on the basis of being the intimate partner of a person with cancer. Demographic details of the sample are presented in Table 1. For 8 of the 156 partner carers, the cancer type and status of the cancer were not reported in their questionnaire responses. Of the 46% partner carers who indicated a willingness to be interviewed about sexuality, 20 were selected for interview on the basis of reporting changes to sexuality since the diagnosis of their partner's cancer, with the sample stratified by gender, cancer stage, and type.
Table 1. Sample Characteristics for Partner Carer and Person With Cancer
The larger study examining the needs and concerns of informal cancer carers in New South Wales, Australia, from which the participants were drawn, was advertised via cancer and carer-specific newsletters, Web sites, and organizations, as well as through media releases, cancer support groups, and cancer clinics across New South Wales. Family members, partners, or friends of people with cancer who self-identified as providing care and who volunteered to take part in the research were sent an information sheet, consent form, questionnaire, and interview contact form. Ethical approval was granted from all relevant committees including 10 Area Health Services across New South Wales, the Cancer Council New South Wales, and the University of Western Sydney.
Measures
Questions on sexuality were developed for the study in consultation with the study's steering advisory committee, which was composed of 2 carer representatives from an independent advocacy organization (Cancer Voices New South Wales), professionals providing support services to cancer patients and their carers, an oncologist, and researchers working in the field of psycho-oncology, sexuality, health, and gender. Three fixed-choice questions (no, yes) asked the participants whether they were in a sexual relationship with a person with cancer, whether there had been changes to their sexual relationship after cancer, and whether issues about sexuality had been discussed with a healthcare provider. The 2 open-ended questionnaire items concerning changes in sexuality after cancer were the following: please describe the changes to your sexual relationship and if your role as carer has made any difference to your sexual relationship, please describe this difference.
A semistructured interview, audiorecorded and conducted on a face-to-face or telephone basis lasting approximately 1 hour, was used to examine in depth partners' experiences of sexuality after cancer. The interview discussion focused on changes to partners' intimate/sexual relationship, feelings about their intimate/sexual relationship, communication with the person with cancer about intimacy, and experiences with healthcare professionals. In accordance with established protocols in qualitative research, sampling was discontinued when information redundancy was reached, and no additional information was forthcoming. [25]
Analysis of Open-Ended Questions and Interviews
All of the interviews were transcribed verbatim, and thematic analysis was used to analyze the data. [26] After transcription, the interviews and open-ended questionnaire responses were independently read by 2 researchers to ascertain the major themes and develop a coding frame. Following a discussion between the researchers and other members of the research team, the coding system was used to organize the data into conceptual categories, which were based on participants' stories and responses. The research was, therefore, largely inductive, in which the concepts and categories came from the data, rather than being deductive or informed by existing preconceptions about cancer caring and sexuality. [27] The interpretation of the data was conducted from within the framework of positioning theory, [28] where it is assumed that narratives do not simply mirror a world "out there" but that they are constructions that reflect subject positions taken up or given to individuals, which provide the context for the negotiation of experience. The interviews and responses were then coded thematically by 2 of the researchers using consensus discussion, with a third researcher available to discuss any disagreements (which rarely arose). NVivo software, a program by QSR International ( Australia) that allows for qualitative data to be organized thematically, as well as across demographic or other key variables, was used to organize the coded data. The coding frame focused on the following major themes: nature of changes to sexuality (cessation, reduction, renegotiation), reasons given for changes to sexuality (impact of cancer or cancer treatment: caring role, repositioning of person with cancer as patient), and feelings about such changes (positive and negative). Discussion and competing explanations between the 2 researchers during the coding process and discussions with the broader team allowed the coding frame to be refined. [29] Responses from the questionnaire were also tabulated and counted to identify frequency and patterning within and across groups, specifically gender and cancer type.
Results
One hundred twenty-two participants (43 men, 79 women), or 78% of this subsample, reported that the onset of cancer had negatively impacted upon their sexuality and their sexual relationship. When we examined the type of cancers associated with changes to sexuality after cancer, the rate was 90% for partners of men with prostate cancer, 71% for partners of women with gynecologic cancer, and 78% for partners of women with breast cancer. Overall, the percentage of partner carers of partners with "nonreproductive" cancers who reported an impact on the sexual relationship was 76%, and the percentage of those caring for partners with cancers involving reproductive sites was 84%.
Each of the 122 participants elaborated on the changes to his or her sexual relationship experienced after cancer in open-ended responses. These responses concerned the status of the sexual relationship, perceived reasons for the changes, and partners' feelings about the changed relationship. Each theme is reported below, illustrated by extracts from the open-ended questionnaire items and the interviews. Demographic information is provided for longer quotes stemming from the interviews. For readability, these specific details are not provided for every open-ended questionnaire quote. Percentages cited refer to the open-ended questionnaire responses.
Status of Current Sexual Relationship
Two major themes characterized accounts of the current status of the sexual relationship: cessation or decreased frequency of sex or intimacy and renegotiation of sex or intimacy.
Cessation or Decreased Frequency of Sex and Intimacy. A complete cessation of sex or a marked decrease in the frequency of sex was reported by 59% of the women and 79% of the men. For those who experienced a complete cessation of sex, the "end" of the sexual relationship was reported as a sudden event: "[o] ur sex life disappeared overnight" and "[g]one from fantastic sex life to none." For other participants, it was a gradual change: "[i]nitially we found other ways to be intimate, however, over time our sex life has ceased." The impact of both the cessation of sex and the loss of intimacy was evident in the following interview extract:
A big... big chunk of your life is lost, and I don't just mean the physical aspects of it... I mean that's... you can live with that or you can... or go without, but... the whole package is gone and I think that's hard that, you're a widow with somebody that's still around. [57-year-old woman caring for 53-year-old husband with brain cancer]
Of the participants who reported decreased sexual frequency rather than a complete cessation, many positioned their sexual relationship in ways that indicated that they had previously enjoyed an active sex life: "[w]e had a very strong physical relationship up until the cancer was discovered and after it, it just faded away" and "[v]ery poor, we use to have sex 5 times a week, now maybe once in 3 or 4 months." Others simply described a change in frequency: "[v]irtually non-existent" and "[t]his aspect of our marriage has nearly stopped." Many of the participants who reported cessation or decreased frequency of sex also reported decreased closeness and intimacy. Responses included the following: "I couldn't cuddle like we used to" and "[o]ften feel frustrated that it doesn't happen like it used to-he is not as romantic either."
Renegotiation of Sexual and Nonsexual Intimacy After Cancer. A renegotiation of their sexual relationship to include noncoital sexual practices or the development of nonsexual intimacy was reported by 19% of the women and 14% of the men. Men (12%) were more likely than women (1%) to report having developed alternative sexual behaviors to those practiced before the patient had cancer. These behaviors consisted of changed sexual positions when attempting intercourse: "I am obviously more careful, having adjusted positions," and the development of "workable alternatives to achieve partner satisfaction... within restrictions caused by the treatments," including oral sex, massage, masturbation, or the use of a vibrator.
Women (18%) were more likely than men (5%) to report that renegotiation involved nonsexual intimacy such as hugging and cuddling: "I'd put my legs up on his lap, and he'd put his arms around me, and I'd cuddle into him, and we'd watch TV."
The last week of my husband's life, he wanted to make love, but physically could not due to his illness. We talked this over as we always did and he knew that hugs, cuddles, and closeness were far more important than the actual act of making love. [64-year-old woman who cared for 64-year-old husband with pancreatic cancer, bereaved]
The importance of closeness to the well-being both of the partner and the person with cancer was emphasized by many of the interviewees. In the excerpt below, one partner describes how important it was to maintain physical closeness with her husband, despite the significant physical barriers that could have served to restrict the expression of intimacy.
We deliberately had kept the double bed. And then, when he got sick, and they needed a more supportive bed, I brought my single bed in, and we got this special height, set at the same height, so that he was always next to me.... I remember the morning he died, I remember cuddling him all night. (...) Just to have your... to have your arm around him was just so, so good. [59-year-old woman who cared for 69-year-old husband with mesothelioma, bereaved]
Reasons for Changes in Sexual Relationships
Many of the participants provided reasons for changes in their sexual relationship after cancer including most notably the impact of cancer treatment, exhaustion resulting from the caring role, and repositioning of the person with cancer as a patient rather than as a sexual partner.
Impact of Cancer Treatment. Cancer treatments were positioned as the primary reason for changes to the sexual relationship. The effects of the treatments meant that there were now physical barriers to sex, which were reported by 30% of the men and 33% of the women. For example, "[h]ormonal treatment has the effect of chemical castration, ie, my husband has no sexual function"; "her poor body has been so cut and chemo has affected her so much that sex is not even possible"; and "non-existent due mainly to the chronic pain syndrome and a less than full confidence in colostomy bags!" For others, cessation or reduction in sex was due to overall bodily restrictions: "[h]e is physically unable to position himself for sex now."
In June an epidural catheter was inserted into my husband's chest and commenced on morphine 30 mgs three times a day. Not only was there no energy or inclination, because of the pain and reduced energy, there was now a "physical barrier" to our relationship as well as all the side effects of morphine. [59-year-old woman who cared for 56-year-old husband with mesothelioma]
Many of the participants also described adverse effects of the treatment such as pain, fatigue, and exhaustion. As one woman participant said about pain, "[w]hen he is unwell because of treatment I tend to be very careful in touching him in case it causes further pain/discomfort." Descriptions of fatigue being given as a reason for changes to the sexual relationship included the following: "[a]s a result of treatment (chemotherapy) my wife is tired more of the time and her libido is reduced" and "[h]e was just too exhausted." The impact of cancer treatment on the self-esteem and self-image of their partner was also identified as a reason for changes to the sexual relationship in a number of cases. For example, one partner commented:
As her health declined she had very low self-esteem caused by loss of hair and muscle tone. When I did have sex at the beginning she would accuse me of not treating her the same as I did in the past and get depressed. [61-year-old man caring for 43-year-old female partner with lung cancer, bereaved]
Exhaustion Resulting from the Caring Role. Exhaustion resulting from the caring role was positioned as the cause of changes to their sexual relationship by 16% of the women and 9% of the men. The responses included the following: "[w]e don't really have any intimacy anymore for reasons including his health and my exhaustion"; "[e]xhaustion, brain still ticking about things to be organized"; and "[e]ven if he was still interested in the sexual side of our marriage I think I would have been too exhausted to have taken part." Participants also commented on a revised prioritization that centered on coping and survival, leaving no time for sex or intimacy.
The sexual issue is really not a priority as all our energy seems to be focused on trying to find a way to beat the cancer. [44-year-old woman caring for 58-year-old husband with prostate cancer]
The Repositioning of the Person with Cancer as a Patient. For 28% of the women and 47% of the men caring for a partner with cancer, the caring role was reported to have resulted in a repositioning of the person with cancer as a patient, which subsequently influenced their sexual relationship. Many partners described emotional effects of the caring role or concern for their partner's feelings and health status. Comments included the following: "[w]ith all the worry and stress that my husband is most likely to die, I now have very little desire for sex"; "[c]urbed by concerns about inflicting pain or discomfort"; and "I just wanted to treat her the same as I always did but I couldn't get the thought out of my head that she was terminally ill."
Participants also reported that they had redefined their role as a carer rather than as a "lover." Some examples are as follows: "[m]y role as a carer has overridden my role as a wife..." and "[h]aving to spend more time on house/garden chores and be carer/nurse, one feels more like a housekeeper than a lover."
When you are a carer it's hard to be a lover, for either party, when dealing with incontinence of both bowel and bladder infections, along with the daily grind of showering, dressing, shaving, etc, then transferring from bed to wheelchair and return. [59-year-old woman who cared for 63-year-old male partner with hematologic cancer]
A number of male participants gave accounts that suggested sex was inappropriate with a person with cancer: "I was very aware of my role as carer and never did anything to embarrass my wife. There was never any inappropriate behaviour." This could result in ambivalent feelings in the face of the partners' own desires, as the following account illustrates:
I feel disgusted with myself that I would inflict sex upon a dying woman, having said that my wife does not object and occasionally welcomes it, saying it is a life giving and loving act and a part of our sacrament.... I was never a fast lover, but now I try and get it over and done with for her. [45-year-old man caring for 44-year-old wife with breast cancer]
A number of the women participants also described positioning their partner as a child, a position that was seen as antithetical to sexuality: "it's like looking after... one of your children now."
Partners' Feelings About Their Changed Sexual Relationship
A number of the participants gave accounts of the emotions that they experienced in response to the changes in their sexual relationship after cancer, with accounts evenly divided between positive and negative feelings.
Positive Feelings. Accounts of positive feelings were provided by 17% of the women and 16% of the men. Many participants described feelings of understanding or acceptance of the effects of cancer or caring on their sexual relationship. Accounts included the following:
Treatment makes my partner feel sick and makes me worry about him so this means we don't feel up to sex... This is not an issue-just a fact/reality of current situation. [39-year-old woman caring for 53-year-old male partner with lung cancer]
He is not up to performing and he has talked to me about it several times, but I assure him that I understand. [66-year-old woman who cared for 66-year-old husband with colon cancer]
A number of participants also reported feelings of affection and companionate devotion:
Sexual urge had gone but my husband made me feel the most loved and cared for woman on this earth by his loving actions, his consideration, his caring attitude and the advice I sought even up till 12 hours before he died. I loved this man totally and he me. [68-year-old woman who cared for 69-year-old husband with brain cancer, bereaved]
[Husband] has multiple brain tumours, lung tumours and clots plus multiple liver tumours so I just hug and reassure that I am here for the "long haul" come what may. [66-year-old woman who cared for 66-year-old husband with colon cancer]
The cancer experience was positioned as having brought the couple closer together by some participants, with one man saying that he "probably has a more affectionate relationship at this point in our lives, and marriage" than before the onset of cancer and another commenting that "with the exclusion of sex, our intimacy is closer probably than it's been for a long time." Increased emotional closeness, despite absence of sex, was also evident in a number of the women participants' interviews:
We are so much closer now than we were... we wouldn't be as close now and we wouldn't be able to talk about absolutely anything now... Just seeing him at night, just makes my heart just go hshshsh... Whereas before I don't think we appreciated that about each other. [29-year-old woman caring for 33-year-old husband with brain cancer]
Negative Feelings. Accounts of negative feelings in response to changes to sexuality were reported by 13% of the women and 21% of the men. These feelings included sadness that their sexual relationship was "lost": "[t]here is just an enormous sadness that we can no longer have this intimacy..." and "[s]till this whole traumatic experience has left me feeling very upset." A number of participants also reported with self-blame, "[n]o sex for 12 months-more my fault," or rejection by their partners, "I felt excluded and unwanted. Sex became a chore and mechanical" and "[s]he has absolutely no sexual interest in me whatsoever."
[S]ometimes you feel guilty that you've got, you know, disgust about it or you know the thing now starts to rot and you feel disgusted by that. [61-year-old woman who cared for 52-year-old female partner with lung cancer]
I don't feel the desire to have a physical relationship with my husband. It almost makes me feel ill to even contemplate it. His whole physical appearance repels me. [52-year-old woman caring for 55-year-old husband with prostate cancer]
A lack of fulfillment in relation to sex was another common feeling: "[n]ot able to relax and enjoy"; "[o]ften feel frustrated that it doesn't happen like it used to"; "[a]t times, I have considered having an affair purely for sexual gratification"; and "leaves me less satisfied." Some participants mentioned feelings of perceived obligation. For men, it was usually in relation to feeling that their partners felt obliged to provide sex. Examples included the following: "[o]n the infrequent occasions we now have sex she wants it over and done with as quickly as possible" and "[s]he became less interested in sex and only accommodated me as if it was a wifey duty." For women participants, obligation was positioned in terms of themselves feeling obliged to engage in sex.
At the early stages of the diagnosis I felt that I couldn't say no to him which put a lot of pressure on me. I had to make sure that I could respond to him and not give him any chance of feeling that I didn't want to make love to him. [59-year-old woman caring for 63-year-old husband with gastric adenocarcinoma]
A small number of women participants shared negative feelings regarding family planning and fertility:
Prostate cancer has required removal of the sac that produces sperm. I am 36 and had always taken for granted I would fall pregnant in the most natural and intimate way. Once my partner is stronger, we will seek advice from an IVF Clinic regarding artificial insemination (hence my partner has secured enough in the sperm bank!). Still this whole traumatic experience has left me feeling very upset. [36-year-old woman caring for 59-year-old husband with prostate cancer]
Discussions of Sexuality With Healthcare Professionals
In response to a question regarding whether a healthcare professional had discussed sexuality with them, 20% of participants indicated that they had. The rate of discussion differed across cancer types, ranging from 50% of prostate cancer partner carers to 0% of respiratory cancer. The rates across the other main cancer types were 33% for brain, 33% for pancreatic, 30% for breast, 29% for gynecologic, 20% for multiple sexual, 17% for colorectal/digestive, 17% for mesothelioma, 15% for multiple nonsexual, 15% for other, and for 9% hematologic. Of those who had discussed sexuality with healthcare providers, only 37% indicated that they were satisfied or very satisfied.
In the interviews, a number of the partners commented on their discussions with healthcare professionals, in each case giving a critical account. When they asked about sexual matters, participants reported being told as follows: "[o]h you don't need to know that and things like that." They were told that they were "irresponsible to be thinking about having children" in raising fertility as a concern. Most, however, gave accounts of sexuality not being discussed at all: "I haven't got a lot of medical advice about how we should continue to conduct our intimate relationship" and "they did not educate us on anything... at all."
[I]t's not properly addressed by the medical profession, it is just completely glossed over. And I can remember, you know, we were sitting when the diagnosis came through and the guy said well, you know, you'll get these hormone pills and we'll give you an injection into your stomach and of course that will be the end of your sex life; and we're just sitting there (...) That was the end of the discussion. [67-year-old woman who cared for 85-year-old husband with prostate, bowel, and lung cancer, bereaved]
Discussion
This study examined changes to sexuality after the diagnosis and treatment of cancer for informal carers who were the partner of a person with cancer. Most participants reported that the cancer experience had impacted on their sexual relationship, resulting in a cessation or reduction of sexual activity, with only a minority renegotiating sexual intimacy after cancer. This supports previous research demonstrating that the impact of cancer and cancer treatment extends beyond the person with cancer, [3-5,7,30] reinforcing the need for acknowledgment of the sexual and intimate needs of partners and of people with cancer. Rather than restricting our sample to partners caring for a person with cancer affecting the reproductive areas of the body, we examined changes to sexuality after cancer across a range of cancer types. Most participants who were providing support to a person with prostate, breast, or gynecologic cancer cited an impact, confirming previous research. [4,13,14] However, the finding that a high proportion of partners of a person with nonreproductive cancer also reported changes highlights the pressing need to acknowledge and attend to the sexual concerns and needs of all partners who care for a person with cancer.
There were some gender differences in the accounts of the nature of changes to the sexual relationship after cancer. Reports of complete cessation of sex were more common for women than for men, and very few women gave accounts of developing alternative sexual practices if intercourse was no longer possible. This could be attributed to women being more likely to assume that they should subordinate their own needs to the needs of their partner [31] and to cultural constructions of normative heterosexuality, which expect men to initiate sex. [32] Previous research has found that partners are reluctant to initiate sexual intimacy if the person with cancer does not initiate [4] and that heterosexual women partners do not wish to initiate sex or discuss alternatives to coital sex for fear of emasculating their partner if he cannot "perform" through sexual intercourse. [33] This is consistent with research that has demonstrated that sexual performance is positioned as central to heterosexual constructions of "manhood," with failure having negative consequences in terms of a man's sense of self. [34] Equally, the "male sex drive discourse," which positions men as "needing" sex, [35,36] may result in the sexual needs of male partners being classified by either or both members of the couple as being "important enough" for sex to continue after cancer or for alternative sexual practices to be developed, in contrast with women partners, who were more likely to report that renegotiated intimacy was nonsexual. The phallocentric bias evident in the research and clinical literature on cancer and sexuality, [37] which serves to reinforce the notion that "normal" sex equals coitus and emphasizes sexual "functioning" with little attention to alternative practices, needs to be challenged, as this potentially plays a significant role in the construction of truths about sexuality, which people with cancer and their partners take up, limiting their exploration of alternatives to coitus after cancer. However, in the present study, 4 of the 6 lesbian partners all reported complete cessation of sex, suggesting that even couples positioned outside of a heterosexual matrix [38] can experience changes to sexuality after cancer.
Although previous research has attributed changes in sexuality and intimacy after cancer to the physiological effects of cancer or cancer treatment, a finding confirmed by many of the accounts in the present study, our findings also showed that the caring role had an impact on the sexual relationship. Participants associated sexual changes with stress, fatigue and exhaustion, revised prioritization centered on coping and survival, and a redefined status as a carer rather than as a lover. Past research that has explored carers' experiences of stress and exhaustion primarily focuses on the impact upon carers' general health and well-being. For example, Brown and Stetz [39] (p186) found that the initial period of "becoming a caregiver" is particularly stressful, as carers not only are focused on their new role but also have to "face the present," negotiate their choice/or lack thereof to care, develop competency around their caring tasks, and evaluate their future. It is important to further investigate how the stresses involved in being a caregiver impact upon a carer's sexuality and how this may in turn impact on quality of life.
The impact of the repositioning of the person with cancer as patient or "child," rather than as "lover," is an important issue that requires further investigation. The finding that the physical symptoms of cancer or the physical tasks associated with cancer caring make it difficult for many carers to continue to see their partner as a sexual person confirms patterns found in other spheres of healthcare. [17] This assignment of individuals with cancer with a "sick" or "childlike" identity, which is antithetical to an identity as a person with sexual desires and needs, can significantly impact on the sexual and intimate relationship of a couple facing cancer. [40] Sex can be positioned as "inappropriate" or as a "frivolous activity," [41] resulting in carers experiencing guilt in the face of their own sexual needs or desires and the avoidance of any discussion or renegotiation of sexual practices, as was reported in the present study. This could be seen as one aspect of a broader practice of self-silencing in cancer carers, where the needs of the carer are repressed because the person with cancer has to be put first. [42] However, it is also associated with cultural discourses that position people with cancer as having limited sexual needs or as asexual, [19,43] resulting in a different set of norms being applied to what is an acceptable behavior. [44] The finding that male partners were more likely to report an impact of repositioning the person with cancer as a patient may result from the role of carer being a more unfamiliar position for men to take up, given the congruence between femininity and the caring role. [31] It may thus be more difficult for men to eroticize a partner with cancer who is in need of care. This matter is worthy of further investigation in future research.
As most partners positioned these changes to their sexual relationship as problematic, confirming previous research, [10,12,15,45] this suggests that education and information about sexuality after cancer, which challenges myths and provides a framework for renegotiation of sexual relationships, need to be included in advice and supportive interventions for partner carers. However, although it has been recognized that healthcare professionals need to discuss issues of sexuality and intimacy with patients in cancer and palliative care [46] and can play a vital role in providing "permission" for sexual intimacy between couples after the onset of cancer by legitimating such discussions, [47] the findings of the present study confirm previous research that found that these discussions are not taking place for most people with cancer or their partners, [48] particularly for those outside the sphere of prostate cancer. Even when sexuality was discussed, this was not at a level that was satisfactory to most participants in the present study. This confirms recent Australian research that reported mismatched expectations and unmet needs in relation to communication about sexuality between healthcare professionals and individuals with cancer, [49,50] suggesting that further education and training of healthcare professionals are required so that they will be able to advise couples affected by cancer on issues of sexuality and intimacy and address their unmet needs in this arena. [51] Although specific interventions have been developed to address sexuality issues in relation to cancer, [52] models of intervention that have been developed for persons with disability [53,54] or individuals who are older aged [55,56] can also be used to facilitate communication about sexuality between couples facing cancer so that they will understand and feel confident about trying "alternative" modes of sexual behavior, such as intimate touching or oral sex, without feelings of guilt or inadequacy. More specifically, couples can benefit from encouragement and permission to raise concerns about sexual functioning, allowing them to ask for and be provided with information within a supportive environment that fosters open communication with healthcare professionals. [52] Strategies that can be used include using normalizing statements to show that discussing sexual issues comprises standard and routine care, adopting a positive attitude toward such discussions, embedding individualized information in other aspects of care, and eliciting basic understanding of concerns and of the individual's motivation to address the issue to offer specific suggestions. [52]
A number of methodological issues need to be considered when evaluating the findings of this research. First, the issue of selection bias must be examined. The present study used self-selection in response to advertisement or information sheets distributed by cancer organizations or clinics and thus may not have tapped a representative sample of informal cancer carers. However, there was a good distribution across cancer type, stage, gender, and age group, in contrast with many previous studies of cancer and sexuality that focused solely on cancers affecting the reproductive organs. Equally, as the participants were recruited for a general study on cancer caring, answering questions on sexuality as part of a broader questionnaire or interview, it could be argued that we have recruited individuals who would not usually respond to requests to take part in a research study on sexuality and thus have obtained a broader sample for our research. Second, this study did not use standardized measures of sexual functioning or sexual or relationship satisfaction but rather focused on subjective reports through open-ended questionnaire items or interview. Future mixed-method research in this field could usefully adopt these standardized measures alongside qualitative measures to allow for greater triangulation of data in evaluating the extent and impact of changes to sexuality after cancer. Third, the cross-sectional design meant that all assessments of change were retrospective. A longitudinal design would more effectively allow for the evaluation of changes to sexuality across cancer stage and allow precancer and postcancer treatment changes to be evaluated more thoroughly.
In conclusion, sexuality and intimacy are central aspects of quality of life that have often been neglected in examinations of the well-being of partners of a person with cancer, particularly for nonreproductive cancers. The findings of the present study add further support to the suggestion that sex should not be positioned as inappropriate or "trivial" in the context of cancer care but rather be recognized as an aspect of couple relationships, which is associated with well-being. [57] Having healthcare professionals legitimate sexuality by "giving permission" for couples to be sexually active or physically intimate when undergoing and recovering from treatment for cancer is one of the key strategies that could assist in this repositioning. [47] The positive consequences of this may include increased feelings of well-being on the part of the partner carer and closeness between the couple, which will have positive consequences for the physical and psychological well-being of the person with cancer, [1] the central aim of professional cancer care. There is thus no justification for sexuality and intimacy being ignored or dismissed; partner cancer carers are telling us that it is important, it is time for healthcare professionals to recognize this need and to act accordingly.
References
- Hodges LJ, Humphris GM, Macfarlane G. A meta-analytic investigation of the relationship between the psychological distress of cancer patients and their carers. Soc Sci Med. 2005;60(1):1-12.
- World Health Organization. The World Health Organisation Quality of Life Assessment (WHOQOL) position paper. Soc Sci Med. 1995;41:1403-1409.
- Juraskova I, Butow P, Robertson R, Sharpe L, McLeod C, Hacker N. Post-treatment sexual adjustment following cervical and endometrial cancer: a qualitative insight. Psychooncology. 2003;12:267-279.
- Maughan K, Heyman B, Matthews M. In the shadow of risk. How men cope with a partner's gynaecological cancer. Int J Cancer Stud. 2002;39:27-34.
- Gurevich M, Bishop S, Bower J, Malka M, Nyhof-Young J. (Dis)embodying gender and sexuality in testicular cancer. Soc Sci Med. 2004;58(9):1597-1607.
- Anderson BL, Golden-Kreutz DM. Sexual self-concept for the women with cancer. In: Baider L, Cooper CL, De-Nour AK, eds. Cancer and the Family. London, England: John Wiley and Sons; 2000:311-316.
- Rolland JS. In sickness and in health: the impact of illness on couples' relationships. J Marital Fam Ther. 1994;20(4):327-335.
- Germino BB, Fife BL, Funk SG. Cancer and the partner relationship: what is its meaning? Semin Nurs Oncol. 1995;11(1):43-50.
- Anllo LM. Sexual life after breast cancer. J Sex Marital Ther. 2000;26:241-248.
- Reichers EA. Including partners into the diagnosis of prostate cancer: a review of the literature to provide a model of care. Urol Nurs. 2004;24(1):22-38.
- De Groot JM, Mah K, Fyles A, et al. The psychosocial impact of cervical cancer among affected women and their partners. Int J Gynecol Cancer. 2005;15:918-925.
- Perez MA, Skinner EC, Meyerowtiz BE. Sexuality and intimacy following radical prostatectomy: patient and partner perspectives. Health Psychol. 2002;21(3):288-293.
- Harden J, Schafenacker A, Northouse L, et al. Couples' experiences with prostate cancer: focus group research. Oncol Nurs Forum. 2002;29(4):701-709.
- Sanders S, Pedro LW, Bantum EO, Galbraith ME. Couples surviving prostate cancer: long-term intimacy needs and concerns following treatment. Clin J Oncol Nurs. 2006;10(4):503-508.
- Kuyper MB, Wester F. In the shadow: the impact of chronic illness on the patient's partner. Qual Health Res. 1998;8(2):237-253.
- Hughes MK. Sexuality and the cancer survivor: a silent coexistence. Cancer Nurs. 2000;23(6):477-482.
- Pope E. When illness takes sex out of a relationship. Siecus Rep. 1999;27(3):8-12.
- Kelly M. Self, identity and radical surgery. Sociol Health Illn. 1992;14(3):390-415.
- D'Ardenne P. The couple sharing long-term illness. Sex Relationsh Ther. 2004;19(3):291-308.
- Butler J. Bodies That Matter: On the Discursive Limits of Sex. New York, NY: Routledge; 1993.
- Gavey N, Mc Phillips K, Braun V. Interruptus coitus: heterosexuals account for intercourse. Sexualities. 1999;2(1):35-68.
- Few C. The politics of sex research and constructions of female sexuality: what relevance to sexual health work with young women? J Adv Nurs. 1997;25:615-625.
- Williams SJ. Beyond meaning, discourse and the empirical world: critical realist reflections on health. Soc Theory Health. 2003;1(1):42.
- Bhaskar R. Reclaiming Reality: A Critical Introduction to Contemporary Philosophy. London, England: Verso; 1989.
- Miles MB, Huberman AM. Qualitative Data Analysis: An Expanded Sourcebook. 2nd ed. Thousand Oaks, CA: Sage Publications Inc; 1994.
- Braun V, Clark JA. Using thematic analysis in psychology. Qual Res Psychol. 2006;3:77-101.
- Janesick VJ. The dance of qualitative research design. Metaphor, methodolatry and meaning. In: Denzin NK, Lincoln YS, eds. Strategies of Qualitative Inquiry. London, England: Sage Publications; 1994.
- Davies B, Harre R. Positioning: the discursive production of selves. J Theory Soc Behav. 1990;20:43-65.
- Barbour RS. Checklists for improving rigour in qualitative research: a case of the tail wagging the dog? Br Med J. 2001;322:1115-1117.
- Walsh SR, Manuel JC, Avis NE. The impact of breast cancer on younger women's relationships with their partner and children. Fam Syst Health. 2005;23(1):80-93.
- O'Grady H. Women's Relationship With Herself: Gender, Foucault, Therapy. London, England: Routledge; 2005.
- Ussher JM. Fantasies of Femininity: Reframing the Boundaries of Sex. London, England: Penguin; 1997.
- Boehmer U, Clarke JA. Communication about prostate cancer between men and their wives. J Fam Pract. 2001;50(3):226-231.
- Tiefer L. The medicalization of impotence: normalizing phallocentrism. Gend Soc. 1994;8(3):363-377.
- Hollway W. Subjectivity and Method in Psychology: Gender, Meaning and Science. London, England: Sage; 1989.
- Potts A. The Science/Fiction of Sex: Feminist Deconstruction and the Vocabularies of Heterosex. London, England: Routledge; 2002.
- Hyde A. The politics of heterosexuality-a missing discourse in cancer nursing literature on sexuality: a discussion paper. Int J Nurs Stud. 2006;44:315-325.
- Butler J. Gender Trouble: Feminism and the Subversion of Identity. New York, NY: Routledge; 1990.
- Brown MA, Stetz K. The labour of caregiving: a theoretical model of caregiving during potentially fatal illness. Qual Health Res. 1999;9(2):182-197.
- Kelly M, Field D. Medical sociology, chronic illness and the body. Sociol Health Illn. 1996;18(2):241-257.
- Holmberg SK, Scott LL, Alexy W, Fife BL. Relationship issues of women with breast cancer. Cancer Nurs. 2001;24(1):53-60.
- Ussher JM, Sandoval M. Gender differences in the construction and experience of cancer care: the consequences of the gendered positioning of carers. Psychol Health. 2008;23(8):945-963.
- Schildrick M. Unreformed bodies: normative anxiety and the denial of pleasure. Womens Stud. 2005;34:327-344.
- Wellard S. Constructions of chronic illness. Int J Nurs Stud. 1998;35:49-55.
- Soothill K, Morris SM, Thomas C, Harman JC, Francis B, McIllmurray MB. The universal, situational and personal needs of cancer patients and their main carers. Eur J Oncol Nurs. 2003;7(1):5-13.
- National Breast Cancer Centre and National Cancer Control Initiative. Clinical Practice Guidelines for the Psychosocial Care of Adults With Cancer. Camperdown, Australia: National Breast Cancer Centre; 2003.
- Schwartz S, Plawecki RN. Consequences of chemotherapy on the sexuality of patients with lung cancer. Clin J Oncol Nurs. 2002;6(4):1-5.
- Stead ML, Brown JM, Fallowfield L, Selby P. Communication about sexual problems and sexual concerns in ovarian cancer: a qualitative study. West J Med. 2002;176(1):18-19.
- Hordern AJ, Street AJ. Communicating about patient sexuality and intimacy after cancer: mismatched expectations and unmet needs. Med J Aust. 2007;186(5):224-227.
- Hordern AJ, Street AJ. Constructions of sexuality and intimacy after cancer: patient and health professional perspectives. Soc Sci Med. 2007;64:1704-1718.
- Rees CE, Bath PA, Lloyd-Williams M. The information needs of spouses of women with breast cancer: patients' and spouses' perspectives. J Adv Nurs. 1998;28(6):1249-1258.
- Hodgkinson K. Addressing sexual and body image concerns. In: Hodgkinson K, Gilchrist J, eds. Psychosocial Care of Cancer Patients: A Health Professional's Guide to What to Say and Do. Melbourne, Australia: Ausmed Publications; 2008:131-145.
- Christopherson JM, Moore K, Foley FW, Warren KG. A comparison of written materials vs materials and counselling for women with sexual dysfunction and multiple sclerosis. J Clin Nurs. 2006;15(6):742-750.
- Simpson G, Anwar S, Wilson J, Bertapelle T. Improving the rehabilitative management of client sexual health concerns after neurological disability: evaluation of a staff sexuality training programme in New Zealand. Clin Rehab. 2006;20(10):847-859.
- Fisher JE, Swingen DN, O'Donohue W. Behavioral interventions for sexual dysfunction in the elderly. Behav Ther. 1997;28(1):65-82.
- Sorocco KH, Kasl-Godley J, Zeiss AM. Fostering sexual intimacy in older adults: the role of the behavior therapist. Behav Ther. 2002;25(1):21-22.
- Cort E, Monroe B, Oliviere D. Couples in palliative care. Sex Relationsh Ther. 2004;19(3):337-354.
-From Medscape Today, http://www.medscape.com/viewarticle/706267_4, retrieved 8/31/09.
9/09