Surviving Critical Illness: Acute Respiratory Distress Syndrome as Experienced by Patients and their Caregivers
Christopher E. Cox, MD, MPH; Sharron L. Docherty, RN, PhD; Debra H. Brandon, RN, PhD; Christie Whaley, BA; Deborah K. Attix, PhD; Alison S. Clay, MD; Daniel V. Dore, Pt, DPT, MPA; Catherine L. Hough, MD, MSc; Douglas B. White, MD, MAS; James A. Tulsky, MD
Posted: 12/21/2009; Crit Care Med. 2009;37(10):2702-2708. © 2009 Lippincott Williams & Wilkins
Abstract and Introduction
Abstract
Objective: To characterize the effects of critical illness in the daily lives and functioning of acute respiratory distress syndrome survivors. Survivors of acute respiratory distress syndrome, a systemic critical illness, often report poor quality of life based on responses to standardized questionnaires. However, the experiences of acute respiratory distress syndrome survivors have not been reported.
Design: We conducted semistructured interviews with 23 acute respiratory distress syndrome survivors and 24 caregivers 3 to 9 mos after intensive care unit admission, stopping enrollment after thematic saturation was reached. Transcripts were analyzed, using Colaizzi's qualitative methodology, to identify significant ways in which survivors' critical illness experience impacted their lives.
Setting: Medical and surgical intensive care units of an academic medical center and a community hospital.
Patients: We recruited consecutively 31 acute respiratory distress syndrome survivors and their informal caregivers. Eight patients died before completing interviews.
Interventions: None.
Measurements and Main Results: Participants related five key elements of experience as survivors of acute respiratory distress syndrome: 1) pervasive memories of critical care; 2) day-to-day impact of new disability; 3) critical illness defining the sense of self; 4) relationship strain and change; and 5) ability to cope with disability. Survivors described remarkable disability that persisted for months. Caregivers' interviews revealed substantial strain from caregiving responsibilities as well as frequent symptom minimization by patients.
Conclusions: The diverse and unique experiences of acute respiratory distress syndrome survivors reflect the global impact of severe critical illness. We have identified symptom domains important to acute respiratory distress syndrome patients who are not well represented in existing health outcomes measures. These insights may aid the development of targeted interventions to enhance recovery and return of function after acute respiratory distress syndrome.Introduction
The acute respiratory distress syndrome (ARDS) is a multisystemic critical illness that affects nearly 200,000 persons in the United States annually. [1] Because ARDS mortality has declined over the past two decades, although its prevalence has not, increasing numbers of survivors are facing significant subsequent critical illness-associated morbidity that may persist for years. [2, 3] Therefore, the use of quality-of-life measures has been encouraged to better understand intensive care unit (ICU) survivors' health outcomes beyond the standard metric of hospital mortality. [4, 5]
To improve ARDS survivors' health outcomes, one must be able to measure these outcomes accurately and comprehensively. Although significant work has documented the long-term outcomes of ARDS survivors and their caregivers using measures of quality of life, to our knowledge, there has been no formal study of ARDS survivors' experiences reported in their own words. [6–9] Therefore, it is not clear what specific aspects of the complex critical illness experience survivors feel are most significant. As a result, outcome measures that do not incorporate ARDS survivors' most important experiences may underestimate both the burden of disease as well as the potential impact of interventions.
We aimed to better understand the experience of ARDS survivors and their caregivers, using a qualitative approach. We conducted semistructured interviews with survivors and their caregivers to assess the experiences as lived by them during the first year after critical care.
Materials and Methods
Study Design
Between June 2006 and June 2007, trained research coordinators screened medical and surgical ICUs daily at Duke University and Durham Regional Hospital for consecutive patients, who required mechanical ventilation and had a Po 2/Fio 2 ratio of < 200. After the primary investigator determined a patient had met the established diagnostic criteria for ARDS, their legal representative was approached for permission to enroll the patient and his/her informal caregiver. [10] Exclusions were lack of identifiable caregiver, lack of English fluency, traumatic brain injury or premorbid cognitive disorder, moribund status, receipt of solid organ transplant, severe chronic obstructive lung disease, and severe burns. Informal caregiver was defined as the person expected to provide the majority of postdischarge patient assistance. The Duke University Institutional Review Board approved the study protocol.
Interviews and Data Collection
Study investigators collected medical chart data including sociodemographics, severity of illness (Acute Physiology and Chronic Health Evaluation II and Sequential Organ Failure Assessment scores), mechanical ventilation parameters, and etiology of ARDS. [11, 12] Semistructured interviews were performed between September 2006 and December 2007. To include a range of the experiences an ARDS survivor might encounter during the year after critical care while focusing on the early dynamic stages of recovery, we randomly assigned participants to be interviewed at 1 to 3 mos (9 [37%]), 4 to 6 mos (5 [21%]), 7 to 9 mos (5 [21%]), and 10 to 12 mos (5 [21%]) after discharge. [9] Enrollment was stopped after thematic saturation was reached as assessed during review of transcripts at 1 yr. [13] In Colaizzi's qualitative methodology, the depth and breadth of information collected are more important than the number of participants. [14]
One investigator (C.E.C.) conducted a separate, semistructured telephone interview with each patient and caregiver that was recorded digitally and subsequently transcribed verbatim by a medical transcriptionist. The primary aim of the interview was to understand the lived experience of critical illness. We began interviews by asking participants to talk about their ICU experiences how they affected their in any way they felt was important. We followed up themes participants raised using specific probe questions as needed for clarification (Appendix).
Coding and Analysis of Interviews
A multidisciplinary group of investigators was trained by experts (S.L.D. and D.H.B.) in the use of Colaizzi's method of qualitative analysis, which employs a structured, multistep, iterative, and inductive approach to describe complex phenomena. [15] Investigators (C.E.C., S.L.D., D.H.B., D.K.A., C.W., A.S.C., and D.V.D.) blinded to participant characteristics each independently analyzed the same six (25%) de-identified patient-caregiver dyad transcripts chosen at random. Each analyst extracted the most significant statements from transcripts and then tried to understand what meaning these statements had about the experience of illness and survivorship. During subsequent analysis meetings, investigators presented their independently formulated meanings and early structure of themes to the group, which then discussed them until reaching 100% agreement. Themes that were initially ambiguous became concrete through this consensus process, resulting in ten themes that were subsequently reviewed by two experts in qualitative methods (D.B.W. and J.A.T.). Based on this feedback, the group collapsed these themes into five final domains. This thematic framework was not further modified significantly during the coding of the remaining 17 patient transcripts.
Interrater Reliability
After the code structure was established, interrater reliability was calculated on a random sample of five (20%) transcripts. The κ statistic comparing the coding of an analyst not involved in the initial theme development (C.L.H.) with that of the PIs (C.E.C.) was 0.81 ( p < .001), representing excellent agreement beyond chance. [16]
Validity of the Findings
To enhance study validity, we shared findings on an ongoing basis with our multidisciplinary team to ensure that the themes generated accurately reflected the participants' statements and seemed compatible with their knowledge of survivors' lived experiences. [17] Also, we recorded a detailed audit trail as themes were developed and organized. The involvement of qualitative experts helped to ensure methodologic rigor. [17] Finally, we incorporated the results of systematic reviews of ICU survivors' quality of life in our probe question outline. [18]
Results
Participants
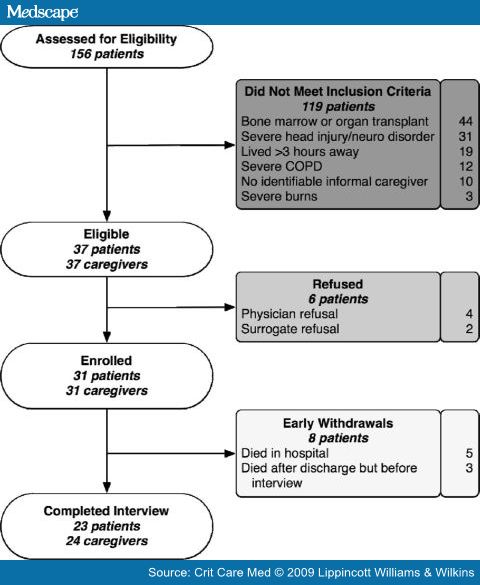
Of 156 screened patients, 119 were ineligible, four surrogates and two physicians refused patient participation, and eight patients died before interviews could be conducted (Fig. 1). The 23 patients enrolled were middle aged, mostly white, insured, and lived at home before hospital admission (Table 1). Most of the 24 caregivers were female and patients' spouses. The patient cohort was diverse in terms of age range, treating service, and ARDS etiology. The median Acute Physiology and Chronic Health Evaluation II score of 23 reflected patients' moderately severe illness. Only eight (35%) patients were discharged home from the hospital, as the remainder was discharged to postacute care facilities. The median time between discharge and interview was 91 days (interquartile range = 37–179 days).
Table 1. Characteristics of patients and caregivers
Characteristic
Patients, n = 23
Caregivers, n = 24
Age
53 (30, 70)
53 (38, 64)
Female
7 (30%)
20 (83%)
Race and ethnicity
White
18 (78%)
19 (79%)
African American
3 (13%)
4 (17%)
Native American
2 (9%)
1 (4%)
Place of residency before admission
n/a
Home
23 (100%)
Caregiver relationship to patient
Spouse or partner
15 (63%)
Child
2 (8%)
Other family member
6 (25%)
Friend
1 (4%)
Insurance status
n/a
Private
13 (57%)
Medicare
4 (17%)
Medicaid
2 (9%)
None
4 (17%)
Location at the time of interview
n/a
Home
22 (95%)
Skilled nursing facility
1 (5%)
Days from discharge to interview
Median, IQR
92 (38–176)
95 (38–142)
Range
19, 337
19, 344
IQR, interquartile range; n/a, not applicable.
Figure 1. Flow diagram of intensive care unit patients screened and enrolled in the study. COPD, chronic obstructive pulmonary disease.
Five central themes emerged from our analysis: 1) pervasive memories of critical care; 2) day-to-day impact of new disability; 3) critical illness defining the sense of self; 4) relationship strain and change; and 5) coping (Table 2).
Table 2. Hospital characteristics and outcomes of patients
Characteristic
Results (n = 23)
ICU admission source, n (%)
Emergency department
14 (61%)
Transfer from outside hospital
8 (35%)
Hospital ward
1 (4%)
Primary admitting service, n (%)
Medicine
10 (43.5%)
Trauma
10 (43.5%)
Surgery
3 (13%)
Etiology of ARDS, n (%)
Pneumonia
7 (30%)
Sepsis
7 (30%)
Contusion
7 (30%)
Aspiration
1 (5%)
Vasculitis
1 (5%)
APACHE II, median (IQR)
23 (20, 27) a
SOFA, median (IQR)
9 (7, 11) a
Charlson score, median (IQR)
0 (0, 2) b
Injury Severity Score, median (IQR)
21 (14, 22) c
Tracheostomy, median (IQR)
13 (59%)
MV days during primary hospitalization, median (IQR)
17 (9, 25)
ICU length of stay, median (IQR)
21 (14, 28)
Hospital length of stay, median (IQR)
27 (21, 42)
Had surgical procedure, n (%)
13 (59%)
Discharge disposition, n (%)
Home independent
5 (22%)
Home with paid care
3 (13%)
Long-term acute care facility
5 (22%)
Skilled nursing facility
4 (17%)
Rehabilitation facility
6 (26%)
ICU, intensive care unit; ARDS, acute respiratory distress syndrome; APACHE II, Acute Physiology and Chronic Health Evaluation; IQR, interquartile range; SOFA, Sequential Organ Failure Assessment; MV, mechanical ventilation.
a Based on ICU day 1 values; b based on comorbidities present before index hospitalization; c for trauma patients (n = 10).Pervasive Memories of Critical Care
Most participants (15 of 23) reported vivid memories of ICU experiences that persisted for months after discharge (Table 3). Many pointed out the seemingly contradictory coexistence of general amnesia regarding their ICU stay with the presence of terrifying dreams, flashbacks, and vivid memories. One patient recalling mechanical ventilation said, "I have memories of jumbled thoughts … it was petrifying. I could hardly tell what was real and what wasn't. This sounds like some kind of novel, doesn't it? Was I dreaming it all?"
Table 3. Themes exemplifying the experiences of acute respiratory distress syndrome survivors
Coded Themes
Examples
Pervasive memories of critical care
It is the same thing over and over—I keep getting moved to different parts of the hospital where my family cannot find me. And then I have experimental [procedures] like students trying to cut me open.
And I still have nightmares or something where I do not know if it was due to the ventilator being put in my throat, or what, but every now and then I feel [something] being pushed down my throat.
Sometimes it just pops into my head, you know. I mean, not [when I am] asleep, just other times around the house—I'm in the hospital again, lying there with people all around me and I cannot move.
Day-to-day impact of new disability
I was like … putty at first. I could not move my hands well at all. There was no feeling in my hands also, like I had been out in the cold for a long time and was clumsy. I could not read a newspaper either. This drove me crazy—this is all an old man has, reading, and I could not focus on the page.
Just could hardly move. I would try to walk across the room, but I had to sit down I was so tired. I'd rest on a chair, then on a couch somewhere else. It took forever to get anything done.
I felt like I was in a cloud or something. I had no attention span. I could not get past two sentences before I was wondering what I was reading—it did not stick. I felt like I was brain damaged.
I cry a lot more than I used to. I'm very emotional now. And the least little thing, I cry. I just sit there and stare at the page … I am paralyzed by inaction.
Critical illness defining sense of self
That has probably been the biggest frustration out of all of this, knowing what I had been capable of and what I'm not capable of doing now, at this point in my life.
It has completely changed my life. I was always the kind of person that was always outside and on the go. Now I cannot do that.
And now here I am. I do not think back on the past much. I am focused on living now. Getting through the day. I am surviving. This is what I've got. It's just … this is all I have to do [now].
Relationship strain and change
[When I was] in the hospital, my brother wasn't able to work. My mama still has to take care of me. She hasn't worked [for 6 mos]. It's a big money thing. I absolutely feel like a big burden on them.
I am dependent on my wife for everything now.
My life is totally changed. I have a husband who cannot function on his own. I have to do everything myself now … I have so much emotion about this, a lot of anger … we are trying to move on. Our relationship will never be the same. It is all gone … different. [ caregiver].
Coping
My work helps a lot, because I just kind of lose myself in what I'm doing. If I hadn't been able to go back to work when I did, it probably would've been much worse than it was.
I got a bunch of friends at work. These guys keep up with me weekly and it's meant a lot to me.
I've rededicated my life to the Lord and got back into church. And I mean, it's turned my life around, really amazingly.
Predominant memories were related to physical restraints, endotracheal tube suctioning, tracheostomies, and an inability to communicate. One pneumonia survivor said: "That was the most troubling thing—when I was awake but could not talk. I was trying to figure out where I was, but it was difficult trying to explain all of this without being able to communicate."
Day-to-day Impact of New Disability
All participants described an often profound and jarring disability that interfered with even basic activities of daily living. Reports of debilitating insomnia, fatigue, tremors, and pain were common. For some, new trauma-associated disability, such as loss of limb and paralysis, superseded all other concerns. However, nearly all reported that weakness was central to their post-ICU experience even months after discharge, as exemplified by a septic shock survivor:
… to start with, when I tried to hold a cup, I spilled it in the bed. I could not brush my own teeth, I could not comb my hair, and I wasn't able to pick the covers up and move them .
Participants also described substantial, persistent cognitive deficits. One caregiver recalled, "It was like I was married to somebody else … he did not remember anything I told him. We went to making lists for everything. I finally told him not to turn on the stove, the washing machine, anything! I was worried he'd burn down the house."
Patients reported symptoms of emotional lability, depression, anxiety, and an enduring sense of fear and foreboding of illness recurrence. The common discordance between caregivers, who described symptoms of significant patient depression and anxiety even requiring medication, and some patients who did not endorse these issues even with probing, suggested widespread symptom underreporting and minimization.
Critical Illness Defining the Sense of Self
Participants (16 of 23) described the transformative effects associated with surviving a debilitating critical illness including new requirements for ongoing medical care, body image alteration by feeding tubes and tracheostomy scars, financial strain, and workplace and family upheaval. One septic shock survivor's simple description exemplified this metamorphosis: "My medical condition is my life now."
Some patients were particularly troubled by a belief that others failed to appreciate their mental or physical transformation by critical illness. One trauma survivor said: "People … sometimes do not know what you go through. They think that because you are in one piece, everything is fine. But inside I'm all screwed up now."
Relationship Strain and Change
Participants (17 of 23) were conflicted in their descriptions of changing social dynamics, intimacy, and relationships. Dramatic and admiring illustrations of the lengths to which family members would go to care for their loved one were common during interviews:
I would have to say it was pretty taxing on my wife. She was going to the hospital at five o'clock in the morning and getting home at two o'clock in the afternoon, probably five out of seven days. Then she picked the kids up and went to work. You know, she's a no-quit kind of person, but I could tell it was hard on her.
However, this caregiving requirement also provoked a sense of guilt, embarrassment, or occasional anger among others—particularly patients who perceived this as role reversal:
It is difficult to be subordinated to everybody I meet or interact with now. Could you imagine what it's like to depend on someone else just to get through the day? To watch my wife get up earlier to fix me up, then go to work, then come back and baby me all over again? Take care of my bandages, my feeding tube, just staring at me like that?
Coping
Most participants (18 of 23) described the importance of finding strategies to adapt to the changes in their lives, such as optimism, hope, support of friends and family, spirituality, antidepressant and anxiolytic medication, self-sufficiency, and setting specific goals like returning to work. Others displayed a remarkable sense of humor about their experience including one elderly trauma survivor who remarked dryly, "The golden years are a bunch of crap!" Many anchored their overall sense of recovery to the nadir of their severe illness experience, tempering their expectations and readjusting their sense of what an acceptable outcome was:
I think [my recovery] went a lot better than what [they] thought because they just kept telling me how amazed they were. And that day that I walked out of the hospital, they all came up from ICU to tell me, 'Bye.' And I walked out! Nobody could believe it .
Some patients, however, reported that they were adjusting poorly to their newly acquired disability. They seemed to deny the majority of their symptoms, perseverate on regrets and missed past opportunities, or profess simple resignation, saying only "this is my life now." One caregiver described the frustrating uncertainty of recovery: "Nobody prepared us for what to expect when we left. When we asked about the quality of life issues, I actually heard one of the doctors say, 'Well, he's alive, is not he?'"
Caregiver Perspective
Although caregivers endorsed the main themes patients described, they also reported unique experiences from their special vantage point (Table 4). Many caregivers (7 of 24) were distressed by fluctuations in patients' mental status and cognition that they felt to be related to medications. The perceived lack of support after leaving the hospital was also stressful. The extent of their postdischarge caregiving strain was notable, as was the emotionally draining experience of explaining the situation to their children as well as balancing child care and work.
Table 4. Representative caregiver interview selections
Caregiver Relationship to Patient
Examples
Wife of patient treated for septic shock
Once we were out of the hospital, we were on our own. Nobody realizes that leaving the hospital is not the end for some people. The next place is just as hard, sometimes worse.
Wife of patient treated for pneumonia
He is better, but I'm exhausted. I am working and then taking care of him and the kids—and we could not get home health care for some insurance reason. Day and night, something is always going on. Nobody could know how bad I have it.
Wife of trauma victim
I could not leave the kids alone at home with him. I was scared he'd do something to them or not be able to watch over them … he is a loving man, but I could not take a chance.
Wife of trauma victim
[Because of his illness] I was out of work for 2 mos [after I had] been placed in charge of a multimillion-dollar project. When I came back, I did not have that project anymore. They seem to have forgotten they promoted me.
Caregivers often identified a sense of increasing distance in their relationships, one saying simply, "I do not think we have a real normal marriage now." Another caregiver explained that financial pressures to return to work also served another purpose: "I hate to say it, but it got me out of the house. It was hard living with him." Although some caregivers described a feeling of irritation or anger with their loved one, a lingering feeling of regret was more common: "You turn around and your life is changed forever." The sense of hopelessness some felt was described poignantly by one:
I feel like I need to be there for him, but he is difficult. I know he is scared, but he doesn't seem to realize how hard on me this is … how hard it is for our kids. I am a nurse and see this every day, but I cannot believe this is happening to me. It is just too much sometimes, overwhelming. What will I do if he gets worse? We are sinking .
Discussion
In this study, we relate, in their own words, ARDS survivors' experiences of being critically ill. Patients reported the recognition of a traumatic event, the change it made in the lives of their loved ones as well as in their own lives, and their attempts to adapt to these changes. Specifically, these interviews with patients and their caregivers demonstrated the pervasive, persistent nature of an acquired disability and its remarkable day-to-day impact on families.
Our work complements past qualitative and quantitative research addressing the outcomes of ICU survivors and their families, allows a better understanding of the specific contributing factors modulating well-being, and touches on new explanatory themes. The ubiquitous presence of physical symptoms, such as weakness in our cohort, was notable, a finding previously described by Herridge and other investigators, although its profound nature and overwhelming importance to nearly every patient was striking—as was patients' relative unpreparedness for its management. [6, 8, 9] Survivors also described relatively unexplored areas of dysfunction, such as disabling insomnia and physical symptoms related to traumatic injury, at the same time rarely endorsing well-studied areas of dysfunction, such as dyspnea. [8, 19, 20]
Past critical care outcomes research has emphasized recall of ICU events and symptoms of posttraumatic stress, as we have done. [21–23] Mechanical ventilation survivors' memories of hospital care were more closely associated with pre-ICU vs. ICU-based events in the qualitative work of Löf and colleagues, although ICU memories dominated among our patients. [24] Roberts and colleagues showed that ICU survivors recalled factual ICU events like an endotracheal tube more readily than imagined experiences, and postulated that early tracheostomy might be less distressing to patients. [25] Jones et al hypothesized that these delusional recollections are more likely than factual recall to lead to traumatic memory acquisition. [26] Patients in our study also reported a predominance of delusional ICU memories, although some tracheostomy tube recipients described this as vividly as those who recalled endotracheal tubes. Overall, patients' psychological distress disrupted their entire families and led to life-changing repercussions.
The high prevalence and persistence of cognitive deficits among ARDS survivors have been described by others including Larson et al and Hopkins et al. [27, 28] However, the deleterious impact of cognitive deficits on patients' daily lives that we observed was underappreciated and sometimes dismissed by physicians, a response that just made things worse.
Our findings give a rich description of a complex experience that may be familiar to providers only in more general terms or as summative questionnaire scores. [29] Regarding the two quality-of-life questionnaires recommended by consensus groups for use among ICU survivors, the Short Form 36 and the EuroQOL 5-D, we have identified potentially modifiable areas of survivors' concern that these questionnaires do not specifically address. These areas include memories of ICU care, personal coping mechanisms, specific physical complaints, issues of changed self-identity, and relationship strain. [5] Although valuable as general measures, our findings suggest that these questionnaires do not allow individuals to specify the unique, important factors affecting their quality of life or to describe the relative importance of these factors.
Finally, these data highlight notable areas for future study and intervention. For example, in addition to efforts to prevent ICU-acquired weakness, easily accessible post-ICU physical rehabilitation programs could offer critical support. [30–32] Behavioral and cognitive therapy interventions targeting coping skills, social support, self-efficacy, and psychological distress have been proven effective in managing symptoms and improving quality of life in other populations, and could be delivered by telephone to these disabled patients who face a long recovery process. [33–38] We urgently need to address family members' dramatic caregiving burden. [39] An equally compelling opportunity for improvement mentioned is the physician-patient/family interaction, described by some study participants as inadequately preparing them for the postdischarge period. [40–42] In summary, we should extend our focus beyond the ICU to attenuate the substantial rippling effect ARDS imprints on the lives of patients, caregivers, and families. [22]
Our study has limitations that may limit its generalizability. Although the number of participants was small and was recruited from only two medical centers, we did observe theme saturation. Only 25% of transcripts were coded by more than one reviewer, although the coding themes were developed by a multidisciplinary team and were applied to a subsequent sample of transcripts with excellent interrater reliability. Our patients were predominantly young, white, male, and had a low premorbid burden of illness. Therefore, our results may not adequately incorporate the unique role expectations and caregiving attitudes of female patients as well as those from different races and ethnicities. Additionally, it is unclear if our findings adequately represent the experience of elderly, more chronically ill persons who may possess a greater burden of postdischarge disability, but though who may also adapt to this burden more readily than younger patients.
Conclusions
Assessing outcomes beyond "28-day mortality," such as quality of life, is an important part of understanding and improving the experience of the expanding number of ICU survivors. Our study has demonstrated that ARDS survivors and their informal caregivers identify many types of experiences that are not well represented on existing standardized measures and that will require different types of interventions to address.
Sidebar
Learning Objectives
After participating in this educational activity, the participant should be better able to:
- Describe the impact of critical illness on quality of care in patients who have survived critical illness.
- Explain the impact of critical illness among caregivers of survivors.
- Use this information in a clinical setting.
The authors have disclosed that they have no financial relationships with or interests in any commercial companies pertaining to this educational activity.
All faculty and staff in a position to control the content of this CME activity have disclosed that they have no financial relationship with, or financial interests in, any commercial companies pertaining to this educational activity.
Lippincott CME Institute, Inc., has identified and resolved all faculty conflicts of interest regarding this educational activity.
Visit the Critical Care Medicine Web site (www.ccmjournal.org) for information on obtaining continuing medical education credit.
Appendix: Protocol for Semistructured Interviews
Introduction
I want to discuss your experience with being very sick and requiring care in an intensive care unit (ICU)-experiences in the hospital and after you left the hospital up until now. But before we begin our discussion, I'd like to review a few things:
- Please say exactly what you think. Do not worry about what I think or what your family or friends think.
- Talk about your experience and feelings, and not about what you have heard others say about this issue.
- Express your opinions truthfully.
- This discussion is being taped, so please speak up and speak clearly.
- Finally, I hope this will be an enjoyable, worthwhile, and stimulating experience.
Today we want to talk about how your ICU experience has affected your life—in any way you think is important. We are interested in finding out what you think either makes your overall satisfaction with your daily life and functioning good or what makes it bad.
General Probe Questions
- How did your ICU experience affect you—in good ways or bad ways? Why?
- What are the most important things to you in your day-to-day life? How did being an ICU patient affect these?
- What are the activities you liked to do in your life that are most important to you? Do you still feel satisfied doing those activities now after your ICU experience?
- How would you describe your quality of life now? Why?
- Has your recovery gone as you expected? Why or why not?
More Specific Probe Questions
- Did you or do you now notice any problems that interfere with your daily routine?
- Do you have worries or concerns about any specific issue now?
- Is your body in the same shape it was before your illness? If not, tell why.
- Have you felt that your emotions are completely normal since your ICU care or serious illness? Why or why not?
- Has your thinking been completely clear since your serious illness?
- Did you go straight home after being in the hospital? If not, what was this experience like?
- How does it feel now that you are at home? Is anything different?
- How important have your friends and family been to you since the hospitalization? Have these relationships changed in any way? If so, why?
- How was your experience in the hospital?
References
- Rubenfeld GD, Caldwell E, Peabody E, et al: Incidence and outcomes of acute lung injury. N Engl J Med 2005; 353:1685–1693
- Cheung AM, Tansey CM, Tomlinson G, et al: Two-year outcomes, health care use, and costs of survivors of acute respiratory distress syndrome. Am J Respir Crit Care Med 2006; 174:538–544
- Rubenfeld GD, Herridge MS: Epidemiology and outcomes of acute lung injury. Chest 2007; 131:554–562
- Rubenfeld G: Looking beyond 28-day all-cause mortality. Crit Care 2002; 6:293–294
- Angus DC, Carlet J: Surviving intensive care: A report from the 2002 Brussels Roundtable. Intensive Care Med 2003; 29:368–377
- Angus DC, Musthafa AA, Clermont G, et al: Quality-adjusted survival in the first year after the acute respiratory distress syndrome. Am J Respir Crit Care Med 2001; 163:1389–1394
- Cameron JI, Herridge MS, Tansey CM, et al: Well-being in informal caregivers of survivors of acute respiratory distress syndrome. Crit Care Med 2006; 34:81–86
- Davidson TA, Caldwell ES, Curtis JR, et al: Reduced quality of life in survivors of acute respiratory distress syndrome compared with critically ill control patients. JAMA 1999; 281:354–360
- Herridge MS, Cheung AM, Tansey CM, et al: One-year outcomes in survivors of the acute respiratory distress syndrome. N Engl J Med 2003; 348:683–693
- Bernard GR, Artigas A, Brigham KL, et al: The American-European Consensus Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med 1994; 149:818–824
- Knaus WA , Draper EA, Wagner DP, et al: APACHE II: A severity of disease classification system. Crit Care Med 1985; 13:818–829
- Vincent JL, Moreno R, Takala J, et al: The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med 1996; 22:707–710
- Sokolowski R: Introduction to Phenomenology. New York, Cambridge University Press, 2000
- Schneider Z, Elliot D, Beounland C, et al: Nursing Research: Methods, Critical Appraisals, and Utilisation. Second Edition. Sydney, Australia, Mosby, 2004
- Colaizzi P: Psychological research as the phenomenologist views it. In: Existential Phenomenological Alternatives for Psychology. Valle RS, King M (Eds). New York, Oxford University Press, 1978
- Sackett DL: Clinical Epidemiology: A Basic Science for Clinical Medicine. Second Edition. Boston, MA, Little, Brown, 1991
- Sandelowski M, Barroso J: Handbook for Synthesizing Qualitative Research. New York, Springer, 2007
- Dowdy DW, Eid MP, Dennison CR, et al: Quality of life after acute respiratory distress syndrome: A meta-analysis. Intensive Care Med 2006; 32:1115–1124
- Cooper AB, Ferguson ND, Hanly PJ, et al: Long-term follow-up of survivors of acute lung injury: Lack of effect of a ventilation strategy to prevent barotrauma. Crit Care Med 1999; 27:2616–2621
- Neff TA, Stocker R, Frey HR, et al: Long-term assessment of lung function in survivors of severe ARDS. Chest 2003; 123:845–853
- Schelling G, Stoll C, Haller M, et al: Health-related quality of life and posttraumatic stress disorder in survivors of the acute respiratory distress syndrome. Crit Care Med 1998; 26:651–659
- Azoulay E, Pochard F, Kentish-Barnes N, et al: Risk of post-traumatic stress symptoms in family members of intensive care unit patients. Am J Respir Crit Care Med 2005; 171:987–994
- Davydow DS, Desai SV, Needham DM, et al: Psychiatric morbidity in survivors of the acute respiratory distress syndrome: A systematic review. Psychosom Med 2008; 70:512–519
- Löf L, Berggren L, Ahlström G: Severely ill ICU patients recall of factual events and unreal experiences of hospital admission and ICU stay—3 and 12 months after discharge. Intensive Crit Care Nurs 2006; 22:154–166. Epub 2005 Oct 28
- Roberts BL, Rickard CM, Rajbhandari D, et al: Factual memories of ICU: recall at two years post-discharge and comparison with delirium status during ICU admission-a multicentre cohort study. J Clin Nurs 2007; 16:1669–1677
- Jones C, Griffiths RD, Humphris G, et al: Memory, delusions, and the development of acute posttraumatic stress disorder-related symptoms after intensive care. Crit Care Med 2001; 29:573–580
- Larson MJ, Weaver LK, Hopkins RO: Cognitive sequelae in acute respiratory distress syndrome patients with and without recall of the intensive care unit. J Int Neuropsychol Soc 2007; 13:595–605
- Hopkins RO, Weaver LK, Collingridge D, et al: Two-year cognitive, emotional, and quality-of-life outcomes in acute respiratory distress syndrome. Am J Respir Crit Care Med 2005; 171:340–347
- Sinuff T, Cook DJ, Giacomini M: How qualitative research can contribute to research in the intensive care unit. J Crit Care 2007; 22:104–111
- Jones C, Skirrow P, Griffiths RD, et al: Rehabilitation after critical illness: a randomized, controlled trial. Crit Care Med 2003; 31:2456–2461
- Rubenfeld GD: Post-hospital case management to improve clinical outcomes in individuals requiring mechanical ventilation (NCT00149513). [cited 2008 August 28] Available from: www.clinicaltrials.gov
- Needham DM: Mobilizing patients in the intensive care unit: Improving neuromuscular weakness and physical function. JAMA 2008; 300:1685–1690
- Blumenthal JA, Babyak MA, Keefe FJ, et al: Telephone-based coping skills training for patients awaiting lung transplantation. J Consult Clin Psychol 2006; 74:535–544
- Lett HS, Blumenthal JA, Babyak MA, et al: Social support and prognosis in patients at increased psychosocial risk recovering from myocardial infarction. Health Psychol 2007; 26:418–427
- Napolitano MA, Babyak MA, Palmer S, et al: Effects of a telephone-based psychosocial intervention for patients awaiting lung transplantation. Chest 2002; 122:1176–1184
- Porter LS, Keefe FJ, Garst J, et al: Self-efficacy for managing pain, symptoms, and function in patients with lung cancer and their informal caregivers: Associations with symptoms and distress. Pain 2008; 137:306–315
- Schnurr PP, Friedman MJ, Engel CC, et al: Cognitive behavioral therapy for posttraumatic stress disorder in women: A randomized controlled trial. JAMA 2007; 297:820–830
- Deja M, Denke C, Weber-Carstens S, et al: Social support during intensive care unit stay might improve mental impairment and consequently health-related quality of life in survivors of severe acute respiratory distress syndrome. Crit Care 2006; 10:R147
- Covinsky KE, Goldman L, Cook EF, et al: The impact of serious illness on patients' families. JAMA 1994; 272:1839–1844
- Curtis JR, Engelberg RA, Wenrich MD, et al: Missed opportunities during family conferences about end-of-life care in the intensive care unit. Am J Respir Crit Care Med 2005; 171:844–849
- White DB, Braddock CH 3rd, Bereknyei S, et al: Toward shared decision making at the end of life in intensive care units: Opportunities for improvement. Arch Intern Med 2007; 167:461–467
- Tulsky JA: Interventions to enhance communication among patients, providers, and families. J Palliat Med 2005; 8 Suppl 1:S95–S102
Authors and Disclosures
Christopher E. Cox, MD, MPH; Sharron L. Docherty, RN, PhD; Debra H. Brandon, RN, PhD; Christie Whaley, BA; Deborah K. Attix, PhD; Alison S. Clay, MD; Daniel V. Dore, Pt, DPT, MPA; Catherine L. Hough, MD, MSc; Douglas B. White, MD, MAS; James A. Tulsky, MD
Assistant Professor of Medicine (CEC), Duke University, Durham, NC; Associate Professor (SLD), Pediatric Acute/Chronic Care Advanced Practice, Specialty Director, Duke University School of Nursing, Durham, NC; Associate Professor (DHB), Duke University School of Nursing, Durham, NC; Data Technician (CW), Duke University Medical Center, Durham, NC; Director (DKA), Duke Neuropsychology, Duke University, Durham, NC; Assistant Professor of Medicine and Surgery (ASC), Duke University, Durham, NC; Director (DVD), Departments of Physical Therapy and Occupational Therapy, Duke University Health System, Durham, NC; Assistant Clinical Professor (DVD), Duke University Medical Center, Durham, NC; Assistant Professor (CLH), Harborview Medical Center, University of Washington, Seattle, WA; Associate Professor (DBW), Department of Critical Care Medicine, University of Pittsburgh, Pittsburg, PA; Professor of Medicine and Nursing (JAT), Duke University Medical Center, Durham, NC; and Director (JAT), Center for Palliative Care, Veterans Administration Medical Center, Durham, NC.
For information regarding this article, E-mail: christopher.cox@duke.eduThis study was supported, in part, by Grants K23 HL081048 (CEC), K23 HL074294 (CLH), and KL2 RR024130 (DBW) from the National Institutes of Health and Greenwall Foundation Bioethics Faculty Scholars Award (DBW).
The authors have not disclosed any potential conflicts of interest.Crit Care Med. 2009;37(10):2702-2708. © 2009 Lippincott Williams & Wilkins
-From: http://www.medscape.com/viewarticle/711440 retrieved 1/8/10
1/10