From Journal of Pediatric Psychology
The Course of Posttraumatic Stress in Children:
Examination of Recovery Trajectories
Following Traumatic Injury
Robyne M. Le Brocque, PhD; Joan Hendrikz, BSc; Justin A. Kenardy, PhD
Posted: 07/13/2010; Journal of Pediatric Psychology. 2010;35(6):637-645. © 2010 Oxford University Press
Abstract and Introduction
Abstract
Objective Group-based trajectory modeling was used to identify patterns of posttraumatic stress symptom (PTSS) in children 6–16 years following accidental injury. The aims were to: (a) identify probable groups of children following distinct trajectories, and (b) identify risk factors affecting the probability of group membership.
Method Children's Impact of Events Scale ( n = 190) was used to assess PTSS up to 2 years post injury. Age, gender, type of injury, and preinjury behavior were assessed as risk factors.
Results Three distinct trajectory groups were identified: resilient (57%), elevated stress symptoms which recovered quickly (33%), and chronic (10%). Younger children were more likely to be in the recovery group. Those with serious injuries were more likely to be in the chronic group. Preinjury child behavior problems were predictive of recovery and high chronic symptoms.
Conclusion Identification of distinct PTSS trajectory groups has implications for understanding the course and treatment of PTSS in children.Introduction
Accidental injury is one of the leading causes of death and disability in children (World Health Organization, 2006), yet there is a dearth of information on the social and emotional costs resulting from child accidental injury. Posttraumatic stress disorder (PTSD) is a diagnosis used to describe a constellation of child psychological symptoms resulting from exposure to traumatic events including accidental injury. Symptoms include re-experiencing such as flashbacks, avoidance of reminders of the trauma, and increased arousal such as hypervigilance, which persist for over 1 month and cause significant distress or impairment in functioning (World Health Organization, 2006). Subthreshold posttraumatic stress symptoms (PTSS) have also been associated with increased impairment in functioning, and other mental health and behavior problems (Daviss et al., 2000; De Vries et al.,1999). Although varying rates of symptoms have been observed following trauma, few studies have explored individual recovery patterns. This paper explores trajectory patterns of PTSS in children following accidental injury. The relationships between risk factors: child age, gender, type of injury, and pretrauma child behavior and symptom trajectory patterns are examined.
Posttraumatic stress disorder in children following accidental injury has been estimated to be around 20% with an additional 25% of children meeting partial criteria for PTSD (Kahana, Feeny, Youngstrom, & Drotar, 2006). Most studies report a decline in the prevalence of symptoms post injury (Di Gallo, Barton, & Parry-Jones, 1997; Gillies, Barton, & Di Gallo, 2003; Kassam-Adams & Winston, 2004; Mather, Tate, & Hannan, 2003; Max et al., 1998; Olsson, Kenardy, De Young, & Spence, 2008; Sturms et al., 2005). Although the majority of children recover quickly following exposure to traumatic events, there is also evidence that a small minority can develop chronic PTSS (Di Gallo et al., 1997; Gillies et al., 2003; Mather et al., 2003; Pine, Costello, & Masten, 2005). Max et al. (1998) found a pattern of high levels of PTSS up to 3 months posttraumatic brain injury (68%) which declined gradually to 12% at 2 years. While the body of evidence is scarce, some studies have found small numbers of children with delayed onset PTSS (Gillies et al., 2003; Mather et al., 2003; Yule et al., 2000). These cases are more likely to have subclinical symptoms preceding full diagnosis (Yule et al., 2000).
Predictors of PTSS in Children
A number of predictors have been associated with the development of PTSS in children however few studies have explored factors that are associated with improvement or worsening of symptoms over time. Risk factors for PTSS following pediatric accidental trauma have recently been reviewed by Langeland and Olff (2008). These factors include characteristics of the child, such as the child's previous trauma experiences and coping (Daviss et al., 2000; Max et al., 1998; Stallard, 1999); characteristics of the event and resulting injury, such as the mechanism of injury and the type of accident (Stallard, 1999), the type and severity of injury (De Vries et al., 1999; Kassam-Adams & Winston, 2004; Landolt, Vollrath, Ribi, Gnehm, & Sennhauser, 2003; Max et al., 1998); the psychological and biological responses of the child at the time of trauma, such as perception of threat (Di Gallo et al., 1997), acute distress symptoms (Daviss et al., 2000; Di Gallo et al., 1997; Max et al., 1998; Meiser-Stedman, Yule, Smith, Glucksman, & Dalgleish, 2005), and biological responses to trauma (Kassam-Adams & Winston, 2004; Kenardy, Spence, & Macleod, 2006); and the posttraumatic environment, such as family and social support and parental stress reactions (Daviss et al., 2000; De Vries et al., 1999; Landolt et al., 2003). While results are inconsistent across studies, these factors may be relevant in predicting the course of PTSS over time.
Age and gender have frequently been examined as risk factors for PTSS. Most studies have not found significant effects for gender on child PTSS (Di Gallo et al., 1997; Kahana et al., 2006; Kassam-Adams & Winston, 2004; Olsson et al., 2008). In a meta-analysis by Kahana and colleagues (2006), female gender appeared to increase the risk of PTSS but not PTSD compared to boys. Variable results have also been found for the effect of age on child PTSS following accidental injury, however there is more evidence to suggest that younger children are more vulnerable to PTSD than older children (Di Gallo et al., 1997; Kassam-Adams & Winston, 2004; Olsson et al., 2008). Given the contradictory evidence of age and gender effects on PTSS in injured children, this study examines the relationship of child age and gender and PTSS over time.
The relationship between pre-existing child behavior problems and psychopathology and the development of PTSS is also not well understood. Di Gallo and his colleagues (1997) found that the child's premorbid psychological problems were not related to PTSS. However, they did find that premorbid behavior problems accounted for over 22% of the variance in avoidance symptoms reported at the acute phase. In contrast, Max (1998) found that internalizing disorder at the time of the accident significantly predicted PTSS at 2 years. In addition, Udwin and colleagues (2000) found that mental health difficulties and learning problems in childhood were associated with the development of PTSD including both the severity and duration of symptoms. Because of the inconsistencies in results from previous research, in this paper we examine the effect of child pre-existing behavior problems on trajectories of child PTSS following accidental injury.
Apart from the study by Kassam-Adams and Winston (2004), the few studies that do describe the course of child PTSD and symptoms have methodological limitations, such as a wide range of injuries investigated, small sample sizes, and a variety of instruments for assessing PTSS in injured children, including both diagnostic interviews and self-report questionnaires. This has resulted in variability in diagnosis rates and levels of symptoms reported (Kenardy et al., 2006). Variability in risk factors used to predict PTSD and its symptoms has also been observed. No study to date has explored the impact of these risk factors on the continuance or recovery of PTSS post accidental injury in children.
PTSS Trajectories
To date, studies examining the changes in symptoms over time have been limited to comparison of mean rates (Di Gallo et al., 1997; Gillies et al., 2003) or categorical comparison of symptom severity across data collection points (Kassam-Adams & Winston, 2004; Mather et al., 2003; Max et al., 1998; Sturms et al., 2005). King and her colleagues (2006) used a latent difference score approach to show how more advanced statistical procedures can be used to assess changes in PTSS over time. Higher PTSS scores at admission predicted greater reduction in symptoms by 3 months. Older children were less likely to have a decrease in symptom severity than younger children from 6 to 12 months (King et al., 2006). Advanced statistical modeling tools, such as path analysis and structural equation modeling can be used to explore individual symptom trajectories in more detail. However, only two studies have used growth mixture models to help understand the course of PTSS following trauma (O'Donnell, Elliott, Lau, & Creamer, 2007; Orcutt, Erickson, & Wolfe, 2004). Both studies found two typical symptom trajectories: high levels of symptoms in the acute phase that tended to continue or increase over time and low levels of symptoms that tended to remain low. Only one of these studies focused on PTSS following accidental injury (O'Donnell et al., 2007). Neither explored patterns of PTSD in children.
It is evident therefore that child PTSS may have a variable course over time with symptomatic individuals improving, symptom levels that remain the same over time, and new cases that develop. A useful model to conceptualize the course of PTSS over time can be found in the work of Bonanno and his colleagues, exploring adult adjustment following trauma and bereavement (Bonanno, 2005), and in the work of Layne and his colleagues (2009), exploring risk, vulnerability, resistance, and resilience (Layne et al., 2009). In their work, Bonanno and his colleagues operationally defined four trajectories. Resilient trajectories were characterized by transient, brief, and mild disruption in functioning. Recovery trajectories, in contrast, were characterized by threshold or subthreshold levels of symptoms with significant disruption to daily functioning which resolve to baseline after some months. In addition, they described a group of individuals who appeared to have initially low levels of symptoms but whose symptoms increased over time (delayed symptom trajectory). Finally, individuals with chronic high levels of symptoms post trauma were also identified (Bonanno, 2005). Layne and his colleagues identified a protracted recovery pattern, posttraumatic growth, and a stable maladaptive trajectory (Layne et al., 2009).
Following the models proposed by Bonanno, Layne and their colleagues (Bonanno, 2005; Layne et al., 2009), it is hypothesized that several distinct trajectories of child PTSS will be evident: (a) a resilient trajectory with low symptoms throughout the study, (b) a recovery trajectory with initially high levels of acute symptoms but relatively rapid recovery, (c) a delayed symptom trajectory with low levels of acute symptoms that gradually increase over time, and (d) a chronic symptom trajectory with high levels of acute and ongoing symptoms. To date, there is no evidence relating risk factors as predictors of psychological symptom recovery over time following accidental injury in children. However, it is hypothesized that pre-existing vulnerabilities including pretrauma behavior problems, serious injury, younger age, and female gender will predict the probability of higher initial symptoms and the resulting pathway of recovery.
Methods
Participants and Procedures
Children aged 6–16 years admitted to general or intensive care pediatric units following accidental injury for a minimum overnight stay, and their caregivers, were eligible for the study. After ethical approval from the relevant hospital and University of Queensland review committees, participants were recruited through three tertiary hospitals in Brisbane, Australia. Children with head injuries and those with injuries following interpersonal violence were not included in the study. Potential participants were identified by nursing staff on the wards and referred to the research team. A total of 190 children and their primary caregivers were enrolled in the study. Privacy regulations at this time prevented the collection of information regarding the number or any information about families that did not participate. Children and their parents were recruited within 72 hours after admission. Written informed consent was obtained after complete description of the study to parents and children (if older than 10 years). Time 1 questionnaires were given to parents and children to complete. Clinical interviews were conducted in the family's home at each time point. Questionnaires were also collected at the interview. Child self-report data were collected at a weighted average of 6 days post admission for accidental injury ( n = 175; range 3–14 days). Follow-up data were collected 4–7 weeks ( n = 169; range 28–42 days) and up to 6 months ( n = 158; range 144–172) post injury. A subsample also completed questionnaires 2 years post injury ( n = 51).
Sample Characteristics
Sixty-three percent (63%) of the children were males and the average age of the children at recruitment was 10.7 years ( SD = 2.31; Table I). No data were collected on the ethnicity of the sample however the majority of patients attending the study hospitals (92%) were born in Australia (Dallow, Lang, & Bellamy, 2007). The sample included both life-threatening and relatively benign conditions including: fractures and dislocations, lacerations, burns, internal injuries, foreign objects, and a tooth dislodgement. Some children had multiple injuries. The mean length of stay was 4.2 days ( SD = 6.66 days). The majority of parents and informants completing the questionnaires were mothers (Table I). Most informants were married (74%) and employed (69%).
Table I. Descriptive Statistics
N
%
Mean ( SD)
Min
Max
Total
190
100
Gender
Male
120
63
–
–
–
Female
70
37
–
–
–
Age (years)
190
100
10.7 (2.3)
6.75
16.00
Injury
Fracture/dislocation/laceration/other
166
87
–
–
–
Burns/internal injuries/multiple injuries
24
13
Length of stay in hospital (days)
182
96
4.2 (6.7)
0.33
57.3
Parent informant
Mother
159
84
Father
23
12
Other
8
4
Table I. Descriptive Statistics
N
%
Mean ( SD)
Min
Max
Total
190
100
Gender
Male
120
63
–
–
–
Female
70
37
–
–
–
Age (years)
190
100
10.7 (2.3)
6.75
16.00
Injury
Fracture/dislocation/laceration/other
166
87
–
–
–
Burns/internal injuries/multiple injuries
24
13
Length of stay in hospital (days)
182
96
4.2 (6.7)
0.33
57.3
Parent informant
Mother
159
84
Father
23
12
Other
8
4
Measures
Child acute and PTSS were measured using The Child Impact of Event Scale (CIES) (Dyregrov, Kuterovac, & Barath, 1996; Yule, 1997). The CIES is an eight-item child self-report measure that assesses the effect of trauma, including symptoms of intrusion (intrusive thoughts, nightmares, feelings, and imagery) and avoidance (numbing of responsiveness, avoidance of feelings, situations, and ideas). These items are summed to create a latent measure of Total Subjective Distress. Children were asked to rate the items on a 4-point scale (Not at all = 0, Rarely = 1, Sometimes = 3, Often = 5) according to the frequency with which each symptom had occurred in the past 7 days. The CIES has a range of 0–40. As a screener, the CIES has been found to have excellent sensitivity and positive predictive value, correctly classifying over 75–83% of children diagnosed with PTSD (Perrin, Meiser-Stedman, & Smith, 2005; Stallard, 1999). Confirmatory factor analysis has shown that the two-factor structure is confirmed for children of all ages between 6–15 years (Dyregrov et al., 1996). Reliability of CIES has been reported as moderate to good (Dyregrov et al., 1996; Perrin et al., 2005). In our study, Chronbach's alpha for the total score in the acute phase was 0.84.
Preinjury child mental health was assessed using the Child Behavior Checklist (CBCL) (Achenbach, 1991). The checklist was administered to parents at Time 1 and parents were asked to complete the checklist in relation to their child's behavior prior to the accident. The CBCL consists of 20 social competence and 113 behavioral problem items used to generate broad-band scales of internalizing and externalizing behavior problems. In order to assess clinical significance the scales were converted to T-scores which have excellent reliability and validity (Achenbach, 1991). Items were rated by the parent on a three-point scale indicating if the problem is "very/often true", "somewhat or sometimes true", or "not true". Extensive studies have been conducted to establish the external validity, cross-cultural validity (including Australian norms), and reliability of the CBCL (Achenbach, 1991). The internalizing and externalizing constructs were used in this study.
Due to low cell numbers, injury type was grouped into two categories (Group 1: fracture, dislocations, lacerations, and other injuries; and Group 2: burns, internal injuries, and multiple injuries). Hospital length of stay was a contemporaneous factor therefore it was not included in the analysis of risk factors. Preparatory data investigation showed that length of hospital stay was homogenous within the two injury categories, but significantly different between them (Mann–Whitney U-test, Z = –5.755, p < .001). Therefore, the categorization of injury also represents variation relating to severity and subsequent overall hospital experience.
Statistical Methods
Analyses were conducted on 190 cases all of whom had at least 1 data point over the time period. Complete sets of Total Subjective Distress scores at all three time points were obtained for 132 (69.5%) children. With the exception of Total Subjective Distress at 4–6 weeks and 6 months, no significant difference was observed for all other relevant factors and variables between children with complete data and those with incomplete. At 4–6 weeks, those with incomplete data had significantly higher mean distress scores: 13.19 compared to 8.28 for those with complete data, and at 6 months 10.54 compared to 5.90 [ t = 2.7(167), p = 0.008 and t = 2.2(30), p = 0.037, respectively]. The impacts of these differences are addressed in the discussion.
Trajectory analyses A semi-parametric group-based trajectory analytical technique, developed and designed by Nagin and his colleagues (Nagin, 1999), which does not require individuals to have complete outcome records across time,was used to investigate the possibility of four hypothesized clusters of children with different posttrauma longitudinal recovery profiles (trajectories) as measured by the Total Subjective Distress score. For a specified number of underlying latent groups the method uses maximum likelihood to model the probability of group membership, as well as the shape (polynomial parameters) of the trajectories for each group. The iterative procedure fine tunes group membership and the parameters of the trajectories until a criterion of little further change in likelihood is achieved. Different possible models for number of groups and their profiles were compared using the criterion of reasonableness of group size as well as the difference in likelihood expressed as twice the Bayesian Information Criterion (BIC) value (Jones, Nagin, & Roeder, 2001).
Initially, the number of groups that best describes the data was ascertained for quadratic longitudinal profiles. Models consisting of one to seven groups were compared using the criteria. Once the optimum number of groups was ascertained, non-significant higher-order polynomial terms were dropped one at a time for each group and the models compared using the change in twice the BIC. To avoid correlation of polynomial coefficients, the time of assessment (days) was re-coded to center at zero. The censored normal distribution for Total Subjective Distress was assumed. The final symptom profiles (trajectories) were also assessed against the cut-off score of 17 reported by Stallard et al. (1999) indicative of significant PTSS. Observed weighted average scores and predicted scores for each trajectory were plotted against time of measurement up to 6 months. Confirmatory analyses were conducted to include those with records up to 2 years. SAS version 9.1 and the SAS-based procedure PROC TRAJ (Jones et al., 2001) was used for all analyses. All tests were two-tailed and alpha levels of 0.05 used throughout.
The univariate effects of child's gender and age, type of injury, and premorbid behavior on trajectory group membership were examined using trajectory risk factor analyses. The partial effect of significant independent variables was then investigated using a trajectory multiple risk factor analysis. Age was centered at the mean of 10.7 years and internalizing and externalizing T-scores were centered to their means of 50.26 and 53.98, respectively, so that quadratic effects could be investigated. To facilitate explanation, results for continuous variables were expressed as probabilities of trajectory group membership for different values within the range. For the pretrauma internalizing and externalizing CBCL T-scores, those in the range of 60–63 were used to indicate a borderline-problem and scores greater than 63 to indicate a clinical-problem (Achenbach, 1991).
Results
Mean PTSS Over Time
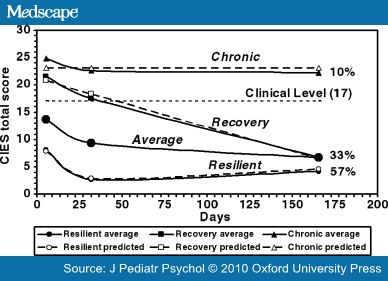
As expected, child PTSS (Total Subjective Distress) showed a marked decline over time since trauma (Figure 1).
Figure 1. Sample mean values and trajectories of weighted average and predicted symptom profiles for Total Subjective Distress symptoms (CIES) up to 6 months post injury.
Trajectory Analysis
Trajectory analyses of Child Total Subjective Distress symptoms following child accidental injury identified three optimum trajectories which were either: (a) well below the clinical level values for the entire period (resilient), (b) above clinical level in the first 4–6 weeks only which then declined to below the clinical level (recovery), or (c) above the clinical level for the entire period (chronic high) (Figure 1). The weighted average Total Subjective Distress score changed by only one or two points at 2 years compared with their score at 6 months. This indicated that these predicted trajectories remained stable over time. As predicted, the majority of children were most likely to belong to a resilient trajectory within normal clinical levels for the entire period (57%) (Table II). The resilient trajectory was quadratic and described a rapid response from slightly elevated symptoms to low levels of distress after 4–6 weeks, which were maintained through to 6 months and 2 years post injury. The recovery trajectory described a steady decline to average levels by 6 months (33%). A constant trajectory described high levels of stress symptoms that change very little over time and remained chronic (10%).
Table II. Trajectory Symptom Profiles for Total Subjective Distress score ( N = 190) a
Time period (months)
Group size (%)
Symptom trajectory
Trajectory polynomials
Brief description b
6
109 (57)
Resilient
Quadratic
Below 17 for entire period
62 (33)
Recovery
Linear
Above 17 for 4–6 weeks and below by 6 months
19 (10)
Chronic
Constant
Above 17 for entire period
24
105 (55)
Resilient
Cubic
Below 17 for entire period
64 (34)
Recovery
Quadratic
Above 17 for 4–6 weeks and below by 6 months
21 (11)
Chronic
Constant
Above 17 for entire period
a Although only 51 children had data to 24 months, all data were included in the analysis in keeping with the fact that data does not have to be complete for the method.
b Clinical cutoff of 17 used (Stallard, 1999).Risk Factor Effects on Symptom Trajectories
In the univariate analyses of Total Subjective Distress, age had a significant linear effect on the probability of membership in the recovery trajectory group compared with the resilient group (Table III) where probabilistically, younger children were more likely to belong to the recovery trajectory group than older children. Children with burns, internal or multiple injuries were significantly more likely to be in the chronic high symptom trajectory group than in the resilient symptom group. In terms of preinjury child mental health, the odds of belonging to either the recovery or chronic trajectory groups compared to the resilient group increased significantly and linearly with both the internalizing and externalizing T-score ( p < .05, Table III). For example, compared to the predicted probability of recovery group membership for an average child (.33), for a child with a borderline-problem internalizing score of 60 this increases to .57. For those with a clinical-problem score of 64 this probability is predicted to increase further to .61. A similar pattern was observed for externalizing behavior problems where the predicted probability of being in the recovery trajectory increased from .33 for an average child to .42 for children with a borderline score of 60, and to .44 for children with a clinical level of 64.
Table III. Univariate Effects of Child's Risk Factors on Child's Group Membership Using Total Subjective Distress
Risk factor
Outcome compared to resilient group
Sample size
Odds ratio
p
Gender
Female (cf. male)
Recovery
190
0.65 (0.27–1.56)
.34
Chronic high
1.10 (0.27–4.49)
.90
Age a
Recovery
190
0.81 (0.67–0.97)
.02
Chronic high
0.86 (0.63–1.16)
.31
Injury
Complex/burns
Recovery
189
1.78 (0.46–6.90)
.41
(cf. fracture, dislocation, laceration)
Chronic high
6.54 (1.41–30.35)
.02
CBCL internalizing
Recovery
174
1.10 (1.04–1.16)
.00
Chronic high
1.12 (1.01–1.26)
.04
CBCL externalizing
Recovery
179
1.05 (1.01–1.10)
.02
Chronic high
1.19 (1.01–1.40)
.04
CBCL: Child Behavior Checklist.
a A quadratic effect was added to the model but it was non-significant.Table III. Univariate Effects of Child's Risk Factors on Child's Group Membership Using Total Subjective Distress
Risk factor
Outcome compared to resilient group
Sample size
Odds ratio
p
Gender
Female (cf. male)
Recovery
190
0.65 (0.27–1.56)
.34
Chronic high
1.10 (0.27–4.49)
.90
Age a
Recovery
190
0.81 (0.67–0.97)
.02
Chronic high
0.86 (0.63–1.16)
.31
Injury
Complex/burns
Recovery
189
1.78 (0.46–6.90)
.41
(cf. fracture, dislocation, laceration)
Chronic high
6.54 (1.41–30.35)
.02
CBCL internalizing
Recovery
174
1.10 (1.04–1.16)
.00
Chronic high
1.12 (1.01–1.26)
.04
CBCL externalizing
Recovery
179
1.05 (1.01–1.10)
.02
Chronic high
1.19 (1.01–1.40)
.04
CBCL: Child Behavior Checklist.
a A quadratic effect was added to the model but it was non-significant.Because the initial internalizing and externalizing scores were correlated (Pearson's r = 0.592, p < .001) two multiple risk factor analyses were conducted to examine the partial effects of age and preinjury behavior. Injury was not included because the reduced sample size resulted in a loss of information that changed some of the injury parameters by over 50% and reversed significance levels. In the multivariate model, the linear effects of the internalizing score and age on the odds of belonging to the recovery compared with the resilient trajectory group retained their significance, as did the effect of internalizing score on the odds of belonging to the chronic high group. However, the effect of externalizing score on the chronic high group compared with the resilient group became non-significant ( p = .06). All odds ratios changed by less than 15%, except for the effect of age on the chronic high symptom trajectory group versus the resilient group which increased by 70% but remained non-significant.
Discussion
This study explored PTSS patterns over time for children after a range of accidental injuries which resulted in admission to hospital. As expected, on average, total symptoms declined rapidly over time. This pattern of decline in overall symptom rates has been observed in studies of both children and adults (Kahana et al., 2006; Mather et al., 2003; Max et al., 1998; Orcutt et al., 2004). However, using more advanced statistical methods three optimum trajectories were found describing children who were resilient to stress following accidental injury and hospital admission (57%), children who exhibited high levels of stress symptoms immediately post trauma but recovered quickly (33%), and children with chronic stress symptoms (10%). These symptom trajectories also reflect patterns described by Bonanno, Layne and their colleagues (Bonanno, 2005; Layne et al., 2009). A majority of children cope well psychologically or recover quickly following accidental trauma and this was supported in our study. However we found a small, but significant group of children who reported ongoing chronic distress. Vulnerable children were more likely to have serious injuries such as internal injuries, burns and multiple injuries, and preinjury behavior problems (Daviss et al., 2000; De Vries et al., 1999; Kassam-Adams & Winston, 2004; Udwin et al., 2000). As missing data were biased toward higher acute symptoms, it is likely that the results relating to chronic symptoms would be conservative. Therefore, more children may be predicted to have a chronic symptom trajectory and the posttraumatic stress symptom levels of the trajectory itself may be higher than reported.
Despite conflicting evidence for delayed onset of symptoms (Gillies et al., 2003; Mather et al., 2003), we found no evidence of trajectories where symptoms emerge at 6 months. Confirmatory trajectory analysis to 2 years also did not reveal evidence of delayed onset. Most studies have found little evidence for delayed onset of PTSS and most examples report subclinical symptoms at earlier phases preceding full diagnosis (Yule et al., 2000). Categorical classification using PTSD diagnoses is useful for showing subjects who move from subclinical to clinical levels of symptoms however this ignores individual variability in symptom presentation. We also found no evidence of symptoms increasing over time as was found in both adult studies (O'Donnell et al., 2007; Orcutt et al., 2004).
Risk analysis showed that age was a predictor of recovery group trajectory membership, with younger children being more likely to have high symptoms immediately post trauma but recovering quickly. Kassam-Adams and her colleagues (2004) also found that younger age predicted earlier symptoms at 1 month but not at 3 months. This suggests that, for younger children, high symptoms post trauma may be a normal reaction and consistent with development. This is in contrast to the study by Dyregrov and his colleagues (1996), who found that younger children reported fewer symptoms than older children.
Preinjury vulnerabilities such as preinjury internalizing and externalizing behaviors also appear to increase the risk of chronic symptom patterns and recovery trajectory patterns post trauma (Daviss et al., 2000; Max et al., 1998). It remains unclear as to whether these vulnerabilities sensitize children with behavior problems to psychological distress following trauma or alternatively if these pre-existing behavior problems are expressed differently (as stress and anxiety symptoms) post accidental injury and admission to hospital. Results indicate that pretrauma behavior and age also have a significant joint partial effect on symptom trajectory membership. In addition, serious internal or multiple injury or burns appear to increase the risk of a chronic symptom trajectory outcome although some studies have found that injury type and severity was not associated with the development of posttraumatic stress (De Vries et al., 1999; Kassam-Adams & Winston, 2004).
The discrimination between children predicted to have a recovery trajectory and those predicted to have chronic symptoms remains an urgent issue. Screening instruments which utilize preinjury behavior, current stress symptoms, and physiological indicators of arousal such as heart rate, may be effective in identifying children who develop chronic PTSS (Olsson et al., 2008). In our study, children who presented with high levels of symptoms in the acute phase, who also had preinjury behavior problems and serious injuries such as burns or internal injuries were more likely to have chronic symptom trajectories. However these same children, but without serious injuries, were more likely to recover. This suggests that early indicators may be used to differentiate children in the acute phase from those who are predicted to recover quickly. Treatment for children can begin earlier if we can identify vulnerable children earlier. In addition, evidence of these two symptom patterns may help explain why acute stress disorder has been found to be a relatively poor predictor of PTSD (Kassam-Adams & Winston, 2004) as only about a quarter of children with high levels of symptoms at the acute phase have chronic symptoms.
There are some limitations in this study. Lack of information about participation rates limits the generalizability of these results. As only a subsample of children were assessed at 2 years ( n = 51), this data were used in a confirmatory analysis to explore symptom trajectories beyond 6 months. However, no changes in symptoms, other than random, were detected after the 6-month follow up. In addition, no data were collected relating to trauma history preadmission. The CIES is an effective screening instrument for PTSD however it does not provide a diagnosis (Perrin et al., 2005; Stallard, 1999). Further research is required using clinician-administered diagnostic interviews. No standardized measure of disability was obtained in this study however further research is required to understand the role of ongoing disability and PTSS trajectories.
Examination of the total number of PTSS over the course of the study identified a decline in mean total symptom levels over time. However, we showed that children's response to traumatic injury is not homogenous and PTSS most likely follow one of several distinct trajectory paths. We found that the majority of children were predicted to have a resilient trajectory of traumatic stress symptoms (57%); about one-third of children were predicted to have initially high symptoms but recovered quickly; and 10% of children were predicted to have a chronic clinical level of stress symptoms. Risk factors for the recovery trajectory group included younger age and preinjury behavior problems. Risk factors for the chronic high symptom trajectory group included serious and complex injury in addition to preinjury behavior problems. Further research is needed to understand the relationship between risk factors and the predicted trajectories, in particular, to differentiate children who have significant distress in the acute phase but recover quickly and those who experience ongoing problems. Secondly, we need to explore the relationship between child and parent PTSS over time. To our knowledge our study is the first to empirically demonstrate that there are three distinct trajectory patterns of children's psychological response to a potentially traumatic event. It provides important information in furthering our understanding of the course of PTSS in children. The ability to identify distinct PTSS trajectories post child trauma and the risk factors for these trajectories has critical implications for the early identification of children who may be at risk. Most importantly, this study demonstrates how the use of advanced statistical modeling can be applied to progress our understanding of the course of psychological symptoms over time for both children and adults for a range of psychopathology.
References
- Achenbach TM. Manual for the Child Behavior Checklist/4–18 and 1991 profile (1991) Burlington, VT: University of Vermont, Department of Psychiatry.
- Bonanno GA. Resilience in the face of potential trauma. Current Directions in Psychological Science (2005) 14:135–138.
- Dallow N, Lang J, Bellamy N. Queensland trauma registry: A summary of paediatric injuries treated in Queensland 2005 (2007) Herston: Centre of National Research on Disability and Rehabilitation Medicine.
- Daviss WB, Mooney D, Racusin R, Ford JD, Fleischer A, McHugo GJ. Predicting posttraumatic stress after hospitalization for pediatric injury. Journal of the American Academy of Child and Adolescent Psychiatry (2000) 39:576–583.
- De Vries A, Kassam-Adams N, Cnaan A, Sherman-Slate E, Gallagher PR, Winston FK. Looking beyond the physical injury: Posttraumatic stress disorder in children and parents after pediatric traffic injury. Pediatrics (1999) 104:1293–1299.
- Di Gallo A, Barton J, Parry-Jones WI. Road traffic accidents: Early psychological consequences in children and adolescents. British Journal of Psychiatry (1997) 170:358–362.
- Dyregrov A, Kuterovac G, Barath A. Factor analysis of the impact of event scale with children in war. Scandinavian Journal of Psychology (1996) 37:339–350.
- Gillies ML, Barton J, Di Gallo A. Follow-up of young road accident victims. Journal of Traumatic Stress (2003) 16:523–526.
- Jones BL, Nagin D, Roeder K. A SAS procedure based on mixture models for estimating developmental trajectories. Sociological Methods & Research (2001) 29:374–393.
- Kahana SY, Feeny NC, Youngstrom EA, Drotar D. Posttraumatic stress in youth experiencing illnesses and injuries: An exploratory meta-analysis. Traumatology (2006) 12:148–161.
- Kassam-Adams N, Winston FK. Predicting child PTSD: The relationship between acute stress disorder and PTSD in injured children. Journal of the American Academy of Child & Adolescent Psychiatry (2004) 43:403–411.
- Kenardy J, Spence S, Macleod A. Screening for risk of persistent posttraumatic morbidity in children following traumatic injury. Pediatrics (2006) 118:1002–1009.
- King L, King D, McArdle J, Saxe G, Doron-Lamarca S, Orazem R. Latent difference score approach to longitudinal trauma research. Journal of Traumatic Stress (2006) 19:771–785.
- Landolt MA, Vollrath V, Ribi K, Gnehm HE, Sennhauser FH. Incidence and associations of parental and child posttraumatic stress symptoms in pediatric patients. Journal of Child Psychology and Psychiatry (2003) 44:1199–1207.
- Langeland W, Olff M. Psychobiology of posttraumatic stress disorder in pediatric injury patients: A review of the literature. Neuroscience and Biobehavioral Reviews (2008) 32:161–174.
- Layne C, Beck C, Rimmasch H, Southwick J, Morena M, Hobfoll S. Promoting "Resilient" posttraumatic adjustment in childhood and beyond: "Unpacking" life events, adjustment trajectories, resources and interventions. In: Treating traumatized children—Brom D, Pat-Horenczyk R, Ford JD, eds. (2009) London and New York: Routledge; Taylor and Francis Group. 13–47.
- Mather FJ, Tate RL, Hannan TJ. Post-traumatic stress disorder in children following road traffic accidents: A comparison of those with and without mild traumatic brain injury. Brain Injury (2003) 17:1077–1087.
- Max JE, Castillo CS, Robin DA, Lindgren SD, Smith WL, Sato Y, et al. Posttraumatic stress symptomatology after childhood traumatic brain injury. Journal of Nervous and Mental Disease (1998) 186:589–596.
- Meiser-Stedman R, Yule W, Smith P, Glucksman E, Dalgleish T. Acute stress disorder and posttraumatic stress disorder in children and adolescents involved in assaults or motor vehicle accidents. American Journal of Psychiatry (2005) 162:1381–1383.
- Nagin D. Analyzing developmental trajectories: A semiparametric group-based approach. Psychological Medicine (1999) 4:139–157.
- O'Donnell ML, Elliott P, Lau W, Creamer M. PTSD symptom trajectories: From early to chronic response. Behaviour Research and Therapy (2007) 45:601–606.
- Olsson K, Kenardy J, De Young A, Spence S. Predicting children's post-traumatic stress symptoms following hospitalization for accidental injury: Combining the child trauma screening questionnaire and heart rate. Journal of Anxiety Disorders (2008) 22:1447–1453.
- Orcutt HK, Erickson DJ, Wolfe J. The course of PTSD symptoms among gulf war veterans: A growth mixture modeling approach. Journal of Traumatic Stress (2004) 17:195–202.
- Perrin S, Meiser-Stedman R, Smith P. The children's revised impact of event scale (CRIES): Validity as a screening instrument for PTSD. Behavioural and Cognitive Psychotherapy (2005) 33:487–498.
- Pine DS, Costello J, Masten A. Trauma, proximity, and developmental psychopathology: The effects of war and terrorism on children. Neuropsychopharmacology (2005) 30:1781–1792.
- Stallard P. Children and young people: The neglected victims of road traffic accidents. In: The international handbook of road traffic accidents and psychological trauma: Current understanding, treatment and law—Hickling EJ, Blanchard EB, eds. (1999) Oxford: Elsevier Science Ltd. 117–127.
- Sturms L, van der Sluis CK, Stewart RE, Groothoff JW, ten Duis HJ, Eisma WH. A prospective study on paediatric traffic injuries: Health-related quality of life and post-traumatic stress. Clinical Rehabilitation (2005) 19:312–322.
- Udwin O, Boyle S, Yule W, Bolton D, O'Ryan D. Risk factors for long-term psychological effects of a disaster experienced in adolescence: Predictors of post traumatic stress disorder. Journal of Child Psychology and Psychiatry (2000) 41:969–979.
- World Health Organization. Child and adolescent injury prevention: A who plan of action 2006–2015 (2006) Retrieved October 10, 2008, from WHO website: www.who.int/violence_injury_prevention/publications/other_injuries/en/index.html.
- Yule W. Anxiety, depression, and posttraumatic stress disorder in children. In: The NFER child portfolio—Sclare I, ed. (1997) Windsor: NFER-Nelson.
- Yule W, Bolton D, Udwin O, Boyle S, O'Ryan D, Nurrish J. The long-term psychological effects of a disaster experienced in adolescence. I: The incidence and course of PTSD. Journal of Child Psychology and Psychiatry (2000) 41:503–511.
Funding
National Health and Medical Research Council of Australia (Grant Number:143021).
Conflict of interest
None declared.Journal of Pediatric Psychology. 2010;35(6):637-645. © 2010 Oxford University Press
Copyright 2007 Society of Pediatric Psychology. Published by Oxford University Press. All rights reserved.
Authors and Disclosures
Robyne M. Le Brocque, PhD, Joan Hendrikz, BSc and Justin A. Kenardy, PhD
Centre of National Research on Disability and Rehabilitation Medicine, Mayne Medical School, University of Queensland
All correspondence concerning this article should be addressed to Robyne M. Le Brocque, Centre of National Research on Disability and Rehabilitation, Medical School, The University of Queensland, Herston Road, Herston 4006, Queensland, Australia. E-mail: r.lebrocque@uq.edu.au-From Medscape Psychiatry, July 20, http://www.medscape.com/viewarticle/724162_6, retrieved 7/21/10.
7/10