|
MGH Community News |
|
MGH Community News |
| March 2016 | Volume 20 • Issue 3 |
Highlights
Sections Social Service staff may direct resource questions to the Community Resource Center, Lindsey Streahle, x6-8182. Questions, comments about the newsletter? Contact Ellen Forman, x6-5807. |
New Immigration Requirements for LIHEAP Fuel Assistance & Season Extended LIHEAP (Low Income Home Energy Assistance Program)—also known as Fuel Assistance—is a federally funded benefit that offers financial assistance to qualifying low-income households who require support in paying their home heating bills. LIHEAP can assist with gas, electric, oil, propane, wood, or coal heating.
Season Extended Immigration Requirements
There is no five year bar or any other special conditions for these qualified statuses. Undocumented immigrants are no longer eligible to receive benefits, but mixed households may receive prorated assistance. A family of four, for example, where three of the members have “qualified alien” status or US citizenship would receive the benefit amount for a family of three. Households whose heat is included in their rent and those living in subsidized housing may qualify if they pay more than 30% of their household income for rent. Homeowners and renters are both eligible. Application |
SNAP ABAWD Time Limit Hitting in April for First Wave of Recipients and Advocacy Tips for Part-Time Workers As reported previously, as of January 1, 2016 for most areas of the state, able bodied adults without children now have to meet work requirements, or face a SNAP 3 month time limit in a 36 month period. DTA was to have started sending out SNAP closing notices to individuals who have not claimed an exemption, have reached their 3 month time limit and do not have any activity that qualifies them for continued SNAP benefits. Known as “able-bodied without dependents” (ABAWDs), these are the individuals age 18 through 49 without disabilities, not living with children and for whom DTA does not have information about possible exemptions. Non-exempt ABAWDS not meeting the work requirements will not get SNAP on their EBT cards in April. MLRI is estimating roughly 10,000 to 12,000 individuals may receive these SNAP closing notices in March. Many clients have received "STRIKE" notices for each month of the 3 months used up.
What you can do for individuals who will be losing SNAP benefits?
What is good cause for not meeting the ABAWD work requirements?
Can an ABAWD get back "retroactive" exemptions to protect their 3 month bucket of benefits?
What if your ABAWD client wants to volunteer somewhere to retain his or her benefits? Advocacy for Those Working Less than 80 Hours a Month What can you do to help ABAWDs with partial earnings keep their SNAP?
What to do if my ABAWD client cannot find any unpaid or volunteer work?
-Adapted from posts to the Food/SNAP Coalition listserv on behalf of Pat Baker, MLRI March 16 and March 24, 2016.
To Keep Health Care Subsidies, Residents Must File Federal Tax Returns State officials and consumer advocates are reminding Massachusetts residents with subsidized health insurance coverage to file their tax returns before April 19 -- or risk losing their federal tax credits. For the first time this year, 174,000 people in Massachusetts who receive tax credits to offset the cost of their health insurance must file a tax form to prove they were eligible for the credits. Those who don’t file could be forced to pay back their tax credits or lose eligibility for credits in future years. Tax credits are available to help individuals and families with low or moderate income pay for health coverage. The new tax rule actually went into effect last year, but because the Health Connector broke down and state officials pushed thousands of people into temporary Medicaid coverage, which is fully paid by the government, the rule affected few people. Many people who have never filed a tax return because they don’t make enough money will have to file this year, state officials and consumer advocates said. Typically, individuals who make less than $10,300 do not need to file federal tax returns.But this year they must file if they earn less than that amount but receive subsidized health coverage, under the federal Affordable Care Act. Louis Gutierrez, executive director of the Massachusetts Health Connector, said the agency mailed notices to remind people receiving subsidized health coverage that they must file tax returns. About 45,000 people who buy insurance on the Connector, but do not receive tax subsidies are not affected by the rule. Volunteers are available to help people file their tax returns. Anyone looking for assistance can call the Internal Revenue Service hotline at 800-906-9887. -See the full Boston Globe article.
Expedited Social Security for Certain Veterans Social Security provides expedited processing of disability benefit applications for wounded warriors and veterans with a U.S. Department of Veterans Affairs (VA) compensation rating of 100% Permanent & Total (P&T). While both Social Security and the VA pay disability benefits to qualifying individuals, the criteria for awarding benefits is not the same. Even if you have a VA compensation rating of 100% P&T, you will need to meet the strict definition of disability set out by the Social Security Act to receive Social Security disability benefits. To receive expedited processing as a veteran rated 100% P&T, you must first apply for Social Security benefits. You can apply online or call the toll-free number, 1-800-772-1213 (TTY 1-800-325-0778). You can also visit your local Social Security office to apply in person. You must identify yourself as a “Veteran rated 100% P&T.” If you apply in person or over the phone, tell the Social Security representative that you are a veteran rated 100% P&T. If you apply online, enter “Veteran 100% P&T” in the “Remarks” section of the application. You must also provide Social Security with your Veterans Affairs notification letter that verifies your rating. Social Security will expedite your claim through the application process, and any appeals level, if necessary. Veterans Affairs compensation will not affect your Social Security benefits. For more information, please visit https://www.socialsecurity.gov/people/veterans/ -Adapted from: http://blog.socialsecurity.gov/social-security-and-the-va-working-together-for-our-heroes/
Arbour Health System Mental Health Hospitals Targeted In Federal Probe The Department of Justice is investigating five hospitals run by the largest private provider of mental health services in Massachusetts for possible billing fraud, according to a report filed recently with the Securities and Exchange Commission. The hospitals are part of Arbour Health System, which is owned by Pennsylvania-based Universal Health Services, the largest owner of psychiatric hospitals and clinics in the country. Over the past three years, the Justice Department’s civil and criminal divisions gradually have expanded their investigations into the company’s facilities across the country. Until now, the only Massachusetts hospital known to be under scrutiny was Arbour-HRI in Brookline. But in the SEC report submitted by Universal, the company revealed that the government’s investigation has grown to cover all of its Massachusetts hospitals, including Arbour Hospital in Jamaica Plain, Arbour-Fuller Hospital in South Attleboro, Pembroke Hospital, and Westwood Lodge. The five hospitals have about 550 beds total and account for more than 20 percent of psychiatric admissions in the state. Arbour also owns outpatient counseling clinics in the state. According to the recent financial filing, more than 25 of the company’s 213 inpatient psychiatric hospitals are under investigation by the federal government. In Massachusetts, Arbour has been cited repeatedly by state regulators over poor care and inadequate staffing at its hospitals and outpatient clinics. At Arbour-HRI two years ago, public health officials found the hospital failed to provide active treatment to some patients, whose diagnoses included bipolar disorder and paranoid schizophrenia. Instead of attending group therapy, inspectors said, patients spent many hours sleeping or wandering the hallways — an allegation the company disputed. This spring, the US Supreme Court plans to review a case brought by the parents of a deceased Massachusetts teenager against Universal Health Services. Yarushka Rivera died soon after receiving care at an Arbour clinic in Lawrence. Her parents contend that the company defrauded government insurance programs by charging for services provided by therapists unqualified to care for their daughter, who was covered by Medicaid. The Service Employees International Union, the nation’s largest health care union with 1.1 million workers, requested in November 2013 that Universal form an independent committee to address patient safety, quality, and compliance at its facilities. Universal declined, said Ryan Pfeffer, SEIU research coordinator. -See the full Boston Globe article.
Woodbriar Nursing Home Residents in “Immediate Jeopardy”; State Blocks New Admits State regulators declared last week that residents at a troubled Wilmington nursing home are in “immediate jeopardy” after a second resident’s death was blamed on substandard care. Officials ordered Woodbriar Health Center to stop accepting new patients, threatened to remove it from government programs that cover most residents’ bills, and recommended fines as high as $10,000 a day until safety is restored.
Woodbriar Health Center was already under investigation after the December death of a patient two days after a staffer accidentally dropped her. “Facilities that fail to protect residents and meet appropriate standards of care will be held accountable,” the state health agency said in a statement. Owners of the nursing home disputed the state’s findings. Investigators discovered issues surrounding the death of the second resident when they visited Woodbriar to determine whether the nursing home had corrected problems uncovered after an earlier resident death, in December. The more recent episode involved a resident who fell out of bed about 9 p.m. Feb. 8 and appeared to have no injuries, according to the state’s letter to Woodbriar. Nursing home workers put the resident back to bed, and contacted a physician who ordered them to check the resident every two hours for signs of medical problems until the next morning, and then check every four hours. But the resident was found dead in bed by 5:30 the next morning, with no record the checks were done as required, according to the state’s letter. “There was no evidence to indicate that following the fall, the facility’s policies and procedures regarding neurological checks were reviewed, and that all staff were trained on assessing and documenting a resident’s status following a fall,” the letter states. Woodbriar is part of a problem-plagued chain of 11 nursing homes owned by Synergy Health Centers, a New Jersey company that has faced mounting citations for substandard care — medication errors, poor infection control, inadequate staff training — since buying its first Massachusetts facility in 2012. A Synergy spokesman Wednesday said in a statement the company “strongly” disagrees with the state’s latest findings, saying the penalties will create “unnecessary confusion and disruption for our residents.” Synergy will appeal the findings while also working with state and federal regulators to resolve the problems, the company said. The state’s letter to Woodbriar said the department is recommending federal regulators impose an immediate financial penalty between $3,050 and $10,000 a day, until the problems are fixed. The state is also recommending Woodbriar be terminated from Medicaid and Medicare, the government health programs that pay its bills, if conditions do not substantially improve by April 14. The immediate steps ordered by the state include a review to ensure all residents are receiving the supervision and care they need to prevent further accidents; a special focus on residents known to be at risk for falls or accidents; and staff training to ensure proper training to respond to residents who fall or are involved in other accidents. -See the full Boston Globe article.
Free Pharmacy Discount Cards – Cost Relief or a Scam? They come unsolicited in the mail or you find a flyer or internet ad advertising significant discounts at the pharmacy. What are pharmacy discount cards? Are the savings for real and what are the risks? The cards claim to offer significant discounts at participating pharmacies. Promotional materials claim different payment sources, typically explaining the savings as volume discounts or payments from the pharmacies as a loss-leader to drive business to their stores. Some journalists and consumers though have posited that an additional, if not the main, way these cards make money is by selling your personal information for marketing purposes. And the up to 50- 75% savings promised? A couple of journalist have consulted pharmacists who said they see various discount cards, which typically provide a price reduction that's less than what you'd get with insurance, but about 10 – 16% off the full retail price. In other words, they could be modestly helpful for those without health coverage. Sources and for more information:
New Law Eliminates License Suspension for Many Drug Crimes Governor Charlie Baker signed legislation this month repealing a 27-year-old law requiring a driver’s license suspension of up to five years for those convicted of drug crimes, such as possession, that have nothing to do with driving. Advocates say the suspensions have been a major impediment for former offenders trying to rebuild their lives. Without a license, it can be difficult to find work, take children to day care, and get to drug-treatment programs. “As the Commonwealth takes important steps to battle substance abuse and reexamine our criminal justice system, I am pleased to sign legislation providing opportunities for those convicted of drug offenses, and who have served their time, to re-enter society, find and keep a job and support their families,” said Baker, in a statement. The current law stems from a 1980s-era get-tough approach to illegal drugs, but critics say it makes it more difficult for offenders who have completed their sentences to get jobs and avoid returning to drugs. The bill also waives a $500 reinstatement fee that drug offenders had to pay to get their licenses back. Judges could still suspend the licenses of people convicted of serious drug trafficking crimes. At a CORI advocacy training attended by CRC staff on Tuesday, Pauline Quiron, director of Greater Boston Legal Services’ CORI and Re-Entry Project noted that the law applies retroactively. The legislation, embraced by law enforcement, passed both the House and Senate unanimously. It is widely seen as the opening salvo in a broader push to overhaul the state’s criminal justice system. Other proposals, like repealing mandatory minimum sentences for drug crimes, face some opposition.
Additional information included as noted.
Cancer Fund of America Declared Sham and Ordered to Dissolve Two nationwide sham cancer charities have been ordered to dissolve, and their president is banned from profiting from any charity fundraising in the future, under a joint settlement reached by Attorney General Maura Healey, along with the Federal Trade Commission and agencies from all 50 states. The settlement, filed Tuesday in the U.S. District Court for the District of Arizona and subject to court approval, resolves claims that the Cancer Fund of America Inc., Cancer Support Services Inc. and their leader, James Reynolds Sr., claimed to help cancer patients, but instead, spent most donations on their operators, families and friends, and fundraisers. The complaint, filed in May 2015, targeted four sham charities run by Reynolds and his family members that allegedly bilked more than $187 million from donors. It was immediately unclear Wednesday how much of that amount came from Massachusetts donors. CFA and CSS were responsible for more than $75 million of that amount. The other two sham charities settled in May 2015. The settlement announced Wednesday concludes the largest joint enforcement action ever undertaken by the FTC and state charity regulators. -See the full The Enterprise article.
Theft of Client Funds from Mental Health Center Due to Inadequate Oversight and Protections Deficiencies in the Gandara Mental Health Center's oversight of client finances, inadequate protections over the agency's own finances, and a lack of supervision on decisions involving staff, board members and related organizations ultimately led to the theft of more than $45,000 in client funds, a state audit released Thursday has found. Massachusetts Auditor Suzanne M. Bump urged the West Springfield nonprofit organization, which contracts with state agencies to provide residential, mental health, and substance abuse-related services to children, adults and families, to strengthen its financial management and improve internal controls.
The audit found that inadequate protections resulted in the theft of client funds, and that Gandara didn't conduct required evaluations of its clients' ability to manage their own money. Bump said Gandara is now following new policies to protect client funds and has fired the employee responsible for the theft. The former employee, whose name was not publicly released, was prosecuted and all clients have since been repaid, Bump said.
MGH Down Syndrome Program The Mass General Hospital Down Syndrome Program integrates state-of-the-art resources with compassionate, comprehensive care through a multi-disciplinary approach. National experts from Massachusetts General Hospital, MassGeneral Hospital for Children, and Massachusetts Eye and Ear Infirmary are ready to help your family member with any medical issue that may occur. Our Down Syndrome Program has five distinct clinical services to ensure that people with Down syndrome receive the specialty care that is specific for their age group:
Services The multidisciplinary team includes a nutritionist and a genetic counselor for pre-natal consultations. Team members include a social worker and psychologist so they are able to assist with educational advocacy and psycho-social issues. They also have a consulting psychiatrist for psychopharmacology. These staffers can also help families and caregivers understand changes in behavior and managing behavior changes. They are also available to consult to inpatient staff Able to consult inpatient for assist to assist in communication, understanding and managing behavior. Tips for Staff
More at: www.massgeneral.org/DownSyndrome
Healthcare Transportation Resources Website The Mass Human Service Transportation (HST) Office hosts a Healthcare Transportation Resources webpage. The site includes many of the resources we already use on a daily basis, but also includes Long-Distance Medical Shuttles and volunteer driver programs. It is always a challenge finding volunteer drivers willing to drive into Boston, but may be worth a try! -Thanks to Lindsey Streahle for sharing this resource.
Senior Medicare Patrol – Fielding Medicare Fraud and Abuse Complaints Senior Medicare Patrols (SMPs) empower and assist Medicare beneficiaries, their families, and caregivers to prevent, detect, and report health care fraud, errors, and abuse through outreach, counseling, and education. SMPs are grant-funded projects of the federal U.S. Department of Health and Human Services (HHS), U.S. Administration for Community Living (ACL). Services provided to the general public include receiving beneficiary complaints. When Medicare beneficiaries, caregivers, and family members bring their complaints to the SMP, the SMP makes a determination about whether or not fraud, errors, or abuse is suspected. When fraud or abuse are suspected, they make referrals to the appropriate state and federal agencies for further investigation.
Source and for more information: http://www.smpresource.org/Default.aspx
Riverside Community Care’s Day Treatment Program Closes – Several Close in Recent Years Riverside Community Care’s day treatment program in Somerville, informally known as the Red House is set to shut its doors after decades of serving people with chronic mental illness. The program fell victim to a collision between soaring real estate prices and inadequate funding of mental health care. The Somerville program is one of two day-treatment programs closing this month in Massachusetts, and at least two others have closed in the past five years — the result, advocates say, of a longstanding failure to invest in outpatient mental health care. “It’s leaving our most chronically ill and most vulnerable patients without their touchstone,” said Jessica Gutchess, the program’s director. Gutchess and others have known for four years they would have to leave the run-down red-shingled Victorian in Davis Square they rented because the building had been sold to a developer to pay off debts. But they held out hope for a new home, until late February when Riverside officials revealed they had failed to find an affordable alternative. On March 4, a similar day treatment program in Roxbury, run by the May Institute, also shut its doors because it was losing money, leaving 25 such programs remaining across Massachusetts. The May Institute and Riverside are coaxing their clients into other day programs in the area or finding other outpatient options, such as individual therapy. But the communities these patients cherished are torn apart. Caitlin Basile said she has not been in the hospital since starting as a patient at the Red House. “It reinforces how invisible we feel in society and how voiceless we are,” said Basile, who suffers from post-traumatic stress disorder, depression, and other conditions. “Now that it’s closing, I feel myself losing a lot of hope.” She has declined to transfer to another day treatment program, not wanting to start over again with a new group that might also eventually have to break up. Thomas Warner feels the same way. The 35-year-old has been coming to the Red House for nine years and believes the relationships he’s developed there are irreplaceable. He credits the day program with keeping him out of the hospital since 2008, even amid his brother’s murder in 2009. Day treatment provides a structure, activities, and a place to socialize for people who might otherwise have no reason to leave home. Some use it to get volunteer or part-time jobs. At the Red House, the schedule includes group meetings focused on issues such as healthy relationships, constructive thinking, and stress management; art, writing, and exercise groups; and casual socializing. Staff members are trained clinicians who turn every encounter into therapy, guiding clients in interpersonal relationships. About 50 clients visit the house over the course of a year, with 18 to 20 in the building on any given day. They attend the program for an average of two years, but some have been coming for decades, Gutchess said. Although they don’t have hard data, people who run the program have no doubt it saves money by preventing hospitalizations. “The situation that developed in Somerville is an example of how precarious these programs are,” said Vic DiGravio, president of the Association for Behavioral Healthcare, a trade group. Funding has long been inadequate for all types of outpatient care, he said. The sad news in Somerville, DiGravio said, comes at a time of otherwise-growing optimism. He said the administration of Governor Charlie Baker has shown it is willing to spend money on behavioral health care. “They’re trying to undo problems that have been developing for 20 years,” he said. Michelle Hillman, spokeswoman for MassHealth, which pays for the care of nearly everyone who uses day treatment programs, said the agency is committed to supporting the programs. This year, MassHealth increased payments for psychiatric day treatment by $500,000, or about 28 percent, for many patients, and is reviewing rates for the others with an eye toward a possible increase July 1. Rates were last increased in 2008. -See the full Boston Globe article.
New MassHealth Prior Authorization Policy for Home Health Services and VNA Referral to ASAPs
As of March 1, 2016, prior authorization is required for all MassHealth Home Health services (skilled nursing, physical therapy, occupational therapy, speech-language therapy, and home health aide services) after a certain number of visits within a specific period depending on the service requested. MassHealth reviews requests for prior authorization on the basis of medical necessity (detailed guidance: Guidelines for Medical Necessity Determination for Home Health Services). These were filed as emergency regulations. There will be a later notice about a comment period.
For continuous skilled nursing services (for more than 2 consecutive hours), PA is required before the provision of services. For therapy services, PA is required as follows.
Agencies do not need to wait until the service thresholds are met before submitting a prior authorization request for continuing services. The MassHealth agency may take up to 14 days to act on a request for prior authorization for continuous skilled nursing services, and up to 21 days to act on a request for prior authorization for all other services. See 130 CMR 450.303(A). If there is an urgent need for prior authorization, the provider should contact the MassHealth Customer Service Center. Providers must submit all information pertinent to the diagnosis using the appropriate Request and Justification form through the Provider Online Service Center (POSC) or by completing a MassHealth Prior Authorization Request form (using the PA-1 paper form and the Request and Justification form) and attaching pertinent documentation. The PA-1 form, the Request and Justification form, and documentation should be mailed to the address on the back of the PA-1 form. Physician Referral and Face-to-Face Requirement As of March 1, 2016, the following requirements apply to physician referrals.
Questions regarding POSC access should be directed to the MassHealth Customer Service Center at 1-800-841-2900. Home Health Agencies Must Refer to Aging Services Access Points Home Health agencies must now refer MassHealth members aged 60 and older to their local Aging Services Access Point (ASAP) upon assessment or reassessment for home health services or discharge from home health services. Sources and for More Information
New MassHealth Opioid and Methadone Prior Authorization requirements The MassHealth Drug List has been amended effective March 7, 2016 to require prior authorization for opioids at lower doses than previously required and for methadone at all doses. Prior authorization (PA) will be required for doses exceeding 120 mg/day of morphine equivalents These doses are available for reference in Table 1 in the MassHealth Pharmacy High Dose letter Methadone will require prior authorization for members considered a new start on the medication (defined as anyone who has not filled methadone for 60 out of the last 90 days). Nationally, methadone accounts for only two percent of opioid pain reliever prescriptions but 30 percent of related overdoses. Because of its drug properties, the risk of overdose from methadone may be disproportionally higher than other pain relievers. These changes are part of a state-wide initiative to address opioid overdoses & deaths. However, for some people experiencing severe pain, the change may present access problems especially during the transition before all prescribers are aware of the new requirements. Remember PA decisions should be made in 24 hours (130 CMR450.303(A), and pharmacies should provide at least a 72 hour supply for a prescribed drug even without PA in an emergency. 130 CMR 406.422(C)--(federal law allows for an exception from the emergency rule for some drugs but not for opioids, see 42 USC 1396r-8(d)(5)). Sources and for More Information
Medicare Reminder – Appealing a Drug Denial If you were denied coverage for a prescription drug, you should ask your plan to reconsider its decision by filing an appeal. Your appeal process will be the same whether you have a stand-alone Part D prescription drug plan or a Medicare Advantage plan that includes your Part D prescription drug coverage. If your pharmacist tells you that your plan will not pay for your prescription drug, you should call your plan to find out the reason it is not covering your drug. Then, you should talk to your prescribing physician about your options. If switching to another drug is not an option, you should file an exception request – a formal coverage request – with your plan. Call your plan to learn how to file an exception request. Make sure you get a letter of support from your doctor and include that with your request. Your plan should issue a decision within 72 hours. File an expedited request if you need your drug right away, and your plan should issue a decision within 24 hours. If your request is approved, your drug will be covered. If it is denied, you should follow the directions on the written denial you receive to appeal. Learn more about this process on Medicare Interactive. Access an interactive roadmap for this process on Medicare Interactive. -From CMS Releases Proposed Changes to MA and Part D for 2017, Medicare Watch, Volume 7, Issue 7, The Medicare Rights Center, March 03, 2016.
Bogus Health Connector Websites The Baker administration has shut down a shadowy commercial website masquerading as the official Massachusetts Health Connector and referring customers to health insurers while collecting a fee in the process. The real Connector is a state clearinghouse for health and dental insurance plans, helping individuals, families, and small businesses secure health and dental coverage. The Connector said the insurance plans it offers receive the state’s seal of approval. The state connector provides outreach through two website addresses, mahealthconnector.org and betterhealthconnector.com. The bogus commercial website, formerly found at healthconnector.co, gave every impression that it was affiliated with the state of Massachusetts. At the top of the home page in large letters was “Mass Health Connector.” Farther down were references to the Massachusetts Health Connector and Health Connector. Only at the bottom of a very long, dense home page was the disclosure that “this website is privately owned and neither affiliated with, nor endorsed by, nor operated by any government agency.” It appears the bogus website was an attempt to siphon off customers headed for the real Connector and refer them to brokers. The state first learned of the bogus website last summer, when the Division of Insurance received complaints from consumers. After consultations with Attorney General Maura Healey’s office, the Connector retained the law firm Mintz Levin Cohn Ferris & Glovsky to shut the website down. Mintz Levin sent a cease-and-desist letter to healthconnector.co in October, accusing the company of attempting to “confuse consumers into believing that your insurance-related services are sponsored, affiliated, or endorsed by our client when, in fact, they are not.” The website did not respond to the letter, so three months later, on Feb. 12, Mintz Levin wrote to GoDaddy, the company that registered the healthconnector.co domain name. GoDaddy promptly suspended the website, and now Mintz Levin is taking additional steps to shut down the website permanently. The Connector may have another problem website on its hands. After the state took action to shut down healthconnector.co, another website operating under the slightly different name health-connector.co was spotted. Calling the number on the website takes you to a company called QuoteWizard, which offers quotes for various types of insurance. State officials could not immediately be reached for comment on the new website. -See the full Commonwealth Magazine article.
Analysis of Proposed Health Safety Net Cuts As reported previously, the state has issued draft regulations which dramatically cut back the Health Safety Net (HSN) which enables free care for people with low-income. The proposed regulation is planned to go into effect no sooner than April 1, 2016 (Health Safety Net Restrictions Planned for April 1st, MGH Community News, February 2016). State senators Jason M. Lewis and John F. Keenan this month sent a letter to Executive Office of Health and Human Services Secretary Marylou Sudders urging her to reconsider the proposed changes. Excerpts of the letter, reprinted below, illustrate the expected impact they would have if enacted: We are concerned that the proposed changes will harm residents who are already medically and socially vulnerable, and the health systems that care for them. We are specifically opposed to the following proposed changes:
The HSN program is an important safety net for uninsured individuals who are categorically ineligible for MassHealth and ConnectorCare, and for underinsured individuals, including low-income seniors. We are especially concerned about the effects of this proposed change on the following low-income populations:
Governor Baker Seeks to Expand Estate Recovery Governor Baker's FY 2017 budget includes a proposal to expand MassHealth estate recovery to include non-probate property. Currently, MassHealth recoups its expenditures from the probate estates of individuals who received coverage of nursing home care or any other MassHealth benefits after age 55. Probate property only includes assets owned by the deceased beneficiary solely in his or her name. Jointly owned property, accounts with beneficiary designations, assets in trust, and real estate in life estates do not pass through probate and are not subject to MassHealth's claim for reimbursement upon the death of the beneficiary.<> In most cases, this expanded recovery would only apply to a beneficiary's home, because few MassHealth beneficiaries have any other significant assets. The proposed law would delay any collection of funds if the property passed to a surviving spouse or to a disabled child, until the spouse or child's death. This Was Tried Before The legislature passed a similar law in 2003 expanding estate recovery to include non-probate property, but then first postponed it and then repealed in 2004 due both to the outcry from constituents where afraid that MassHealth would take their homes and concerns of real estate attorneys that the law would create significant barriers to the sale of real estate. -See the full Margolis & Bloom blog post.
IOM Panel Calls for Training in Social Determinants An Institute of Medicine (IOM) committee is recommending that an understanding of the social determinants of health be incorporated into the education and continuing training of healthcare professionals — and that healthcare professionals also learn how to take action to address issues that can have an outsized impact on their patients' health. "Educating health professionals about the social determinants of health generates awareness of the potential root causes of ill health and the importance of addressing them in and with communities," according to the panel's March 7 report, A Framework for Educating Health Professionals to Address the Social Determinants of Health. If social determinants are not addressed in some way, "the risk of perpetuating a cycle of inequity, disparity, and inequality will remain for generations to come," the report authors write. Although the report is aimed at educators, it contains a call to action for practicing clinicians, said Dr Lane. "Excellent medical care isn't the only thing that creates health," she said. "What creates health is the range of things that people experience in their lives." The report sets up a framework to help the practicing healthcare professional work with the community to address issues such as lack of access to nutritional food or safe housing, said Dr Lane. She points to Mona Hanna-Attisha, MD, as an example of someone who used social determinants to help her patients. The Flint, Michigan, pediatrician was able to trace her patients' high lead levels to a poisoned water supply. "She is a hero," said Dr Lane. "We're not trying to make everybody into a hero, but we're trying to make sure this isn't the one person who has the courage or foresight to be able to do something" by creating a more systemized approach to education. -See the full Medscape article.
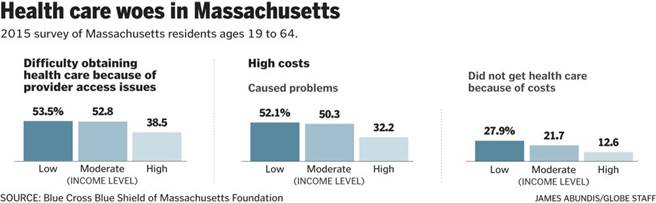
Even with insurance, Mass. residents often can’t afford care Nearly all Massachusetts adults have health insurance, but being insured is no guarantee patients can afford health care or even find someone to provide it, according to a survey released this month. Despite the state’s landmark health care overhaul, the survey by the Blue Cross Blue Shield of Massachusetts Foundation found cost and access remain problems for a significant share of residents, especially those with low incomes or health problems.
More than one-third of adults younger than 65 reported going without needed health care despite having insurance. Nearly half had trouble getting access to a health-care professional. One-fifth struggled to pay family medical bills or medical debts from previous years. The foundation, which has conducted the survey almost every year since 2006, has repeatedly identified these problems. Their persistence echoes difficulties seen nationwide, as medical costs continue to rise and insurance policies require consumers to pay a greater share in deductibles and copays. The proportion of people who had problems paying medical bills has declined slightly since 2006. Still, 43 percent said that in 2015, health care costs had caused problems for them and their families, including 19 percent who went without needed care as a result. The problem was more severe among low- and moderate-income adults and people with health problems. The survey also pointed to problems accessing care. Among adults who had insurance for the entire previous year, 47 percent said they’d had trouble getting in to see a health care professional, because they could not find a provider who accepted their insurance or was accepting new patients, or because they couldn’t get an appointment as soon as needed. This problem has worsened over time. -See the full Boston Globe article.
Hospitals Rattled by Drug Price Increases Doctors at the University Hospitals of Cleveland see an immediately recognizable symbol pop up alongside certain drugs when they sign in online these days to prescribe medications for patients: $$$$$. The dollar signs, affixed by hospital administrators, carry a not-so-subtle message: Think twice before using this drug. Pick an alternative if possible. The Zagat-like approach is just one of the strategies hospitals nationwide are using to try to counter drug costs. It was inspired in part by Shawn Osborne, the University Hospitals system’s vice president of pharmacy services, who saw unexpected price hikes wreak havoc on his budget last year. The increases often involved brand-name drugs with little or no competition as well as commonly used generics around for decades.
Among those tagged were Nitropress and Isuprel, injectable heart medications that are a staple at many hospitals. Their 2015 list prices rose more than 200 percent and 500 percent, respectively, after both were acquired by Canadian-based Valeant Pharmaceuticals.
“There’s been a huge consolidation of these generic companies . . . everybody is buying everybody else,” said Gerard Anderson, a professor at the Johns Hopkins Bloomberg School of Public Health. “If there’s no competition, the prices go up. We are seeing a lot of [drug] shortages, and also price increases. That shouldn’t happen, but it is.” A recent Bloomberg Business survey of about 3,000 brand-name prescription drugs found that prices had more than doubled for 60 medications since December 2014 and at least quadrupled for 20. It found that prices for many other drugs continued to rise at 10 percent or more annually, particularly as competition waned or patents neared expiration. A December report from the Department of Health and Human Services inspector general identified a similar trend. Prices rose faster than inflation for nearly a quarter of top generic drugs between 2005 and 2014, even as prices for many other generics remained low. Nationally, hospitals are aggressively pursuing efforts to anticipate and mitigate drug-cost pressures. Hospital officials insist that even when sudden price increases occur, patients receive access to the medicines they need. But the unpredictable increases wedge their institutions financially, they say: They can’t immediately pass on the cost if a drug gets more expensive because reimbursement rates for certain procedures already have been set by Medicare and private insurers. That means sharply higher prices can lead to losses. And while patients might not feel an immediate impact, down the road they are likely to pay more in insurance premiums and co-payments. The industry, meanwhile, notes that drug spending accounts for only about 10 percent of the country’s health-care costs and that published list prices do not reflect the steep discounts and rebates that companies may offer. Hospitals generally purchase drugs from wholesalers at costs below the list price, although wholesale prices are subject to increases. -See the full Washington Post article.
Mass. Small Business Owners Dropping Health Coverage That’s Become Unaffordable Jon Hurst, president of the Retailers Association of Massachusetts, says his members, which have an average of 10 employees, have seen premiums rise in the range of 12 percent every year for the last decade. “A 12 percent increase in already-high health insurance premiums, coupled with rising rents, rising payrolls and, frankly, sales that are flat or down at the level of inflation, well, that doesn’t work economically — something’s going to give,” Hurst said. “Premiums reflect the cost of medical care,” said Eric Linzer, senior vice president at the Massachusetts Association of Health Plans. “What we’re seeing is a combination of rising prescription drug costs, care delivered in some of the highest-priced settings, and there are significant costs associated with the Affordable Care Act (ACA) that have increased premiums.” Hurst says many small businesses have tried all the solutions brokers suggest, like offering coverage with high deductibles or increasing employee co-pays. Some of the larger small businesses are moving to self-insured coverage, where a company is responsible for the medical expenses incurred by its employees. There are several changes that may have made it easier for workers to move from a company plan to MassHealth (Medicaid) or subsidized coverage through the Health Connector. For one thing, making that transition is now allowed. Before passage of the ACA, Massachusetts residents who had access to insurance through work could not enroll in subsidized plans. But the ACA lifted that restriction and Massachusetts followed suit in 2014. Second, many small businesses no longer face a penalty for failing to provide insurance. A state fee of $295 per worker for firms with 11 or more employees ended in 2013. The state employer penalty for small businesses is scheduled to be replaced this year by a federal fine that applies to some companies with more than 50 workers. Cook, the real estate president, says some companies are splitting in two so that they stay under the 50-worker threshold and avoid the fines. Bill Vernon, Massachusetts director for the National Federation of Independent Business, says members who drop coverage do so because they can no longer afford it. Employees typically switch to a spouse’s health plan, buy coverage on their own or, most commonly, enroll in MassHealth or a subsidized ConnectorCare plan. “People are insured,” Vernon said. “What we see here, I think, is the shift as to who is paying and how it’s being paid.” It’s not clear how big of a shift is underway. Raw numbers from the state Division of Insurance (DOI) show at least a 30 percent drop in small business coverage between 2007 and 2014. But Aron Boros — who directs the Center for Health Information and Analysis — says he can’t tell exactly where employees of small businesses go for insurance if the company ends coverage. Some of the numbers he’s looking at don’t add up. Private plans say they are covering about the same number of people, the state’s uninsured rate was consistent last year at 3.6 percent, and yet enrollment in MassHealth and subsidized ConnectorCare is up. There’s no question this mystery is putting enormous pressure on the state budget. MassHealth grew to just over 2 million residents 15 months ago. That’s one-third of the state’s population. The Baker administration reviewed eligibility and the number dropped to about 1.8 million — still a quarter of all the men, women and children in Massachusetts. State Health and Human Services Secretary Marylou Sudders says she’s not making a direct link between a decline in employer coverage and an increase in the state rolls yet, but is watching the insurance numbers closely. “Massachusetts health reform law is based on all of us having shared responsibility,” Sudders said. “As we go forward we need to be certain that our employers, our individuals and our insurers are all part of that conversation so that we can continue to have 97, almost 100 percent of folks in Massachusetts have health care coverage.” -See the full WBUR Commonhealth blog post.
Governor Baker Signs Opioid Bill In an emotional ceremony, Governor Charlie Baker this month signed into law a measure that places tighter state control on opioids, in an effort to stanch the supply of the addictive drugs. Baker trumpeted the bipartisan legislation as “the most comprehensive measure in the country to combat opioid addiction.” The law will immediately limit initial opioid prescriptions to a seven-day supply. Starting in July, the state will mandate that hospitals administer a substance-abuse evaluation to anyone who shows up in an emergency room believed to be suffering from an opioid overdose. And the new law will eventually require schools to conduct verbal screenings of students for substance abuse. It also requires, starting in October, practitioners check a prescription monitoring program before prescribing drugs that have relatively high potential for abuse. That’s an effort to stop doctor-shopping. And the law allows patients to voluntarily reduce the amount of opioids they receive from a pharmacist, getting, say, 10 pills even if their doctor’s prescription is for 15. While the law is notably weaker than the bill Baker originally proposed — he wanted a three-day initial prescription limit rather than seven, for example — the governor said Monday he signed it happily. Baker had originally proposed allowing hospitals to hold addicts who pose a danger to themselves or others against their will for three days, evaluate them, and decide whether to seek legal permission for longer commitments. The idea was to divert people who might leave the hospital and immediately start using drugs again and allow them to break the cycle of addiction.
But the Legislature balked at the provision, instead putting forward the more modest emergency room substance-abuse evaluation requirement that is now law.
CDC Painkiller Guidelines Aim to Reduce Addiction Risk In an effort to curb what many consider the worst public health drug crisis in decades, the federal government on this month published the first national standards for prescription painkillers, recommending that doctors try pain relievers like ibuprofen before prescribing the highly addictive pills, and that they give most patients only a few days’ supply. The release of the new guidelines by the Centers for Disease Control and Prevention ends months of arguments with pain doctors and drug industry groups, which had bitterly opposed the recommendations on the grounds that they would create unfair hurdles for patients who legitimately have long-term pain. The guidelines are part of a growing backlash against practices developed two decades ago, when doctors across the country began prescribing opioids for routine pain amid claims by pharmaceutical companies and some medical experts that they could be used to treat common conditions like back pain and arthritis without addiction. Those claims ended up in court and were found to be false. Since then, opioid painkillers like OxyContin, Percocet and Vicodin have become the most widely prescribed drugs in the country, with sales of nearly $2 billion a year, according to IMS Health, a research firm that collects prescribing data. But the thinking about the drugs has changed, and the guidelines reflect that. “It has become increasingly clear that opioids carry substantial risk but only uncertain benefits — especially compared with other treatments for chronic pain,” Dr. Thomas R. Frieden, director of the C.D.C., said on a phone call with reporters.“We lose sight of the fact that the prescription opioids are just as addictive as heroin,” he said. “Prescribing opioids is really a momentous decision, and I think that has been lost.” The federal government has lagged the states in its response to the opioid epidemic. Many have already set out rules for doctors to follow, as have some professional medical societies. So proponents of national guidelines applauded their release, which they said was overdue. Although the federal guidelines are nonbinding, they are important because they are now the broadest blueprint in place addressing opioids use. Some observers said doctors, fearing lawsuits, would reflexively follow them, and insurance companies could begin to use them to determine reimbursement. The guidelines recommend what many addiction experts have long called for: that doctors first try ibuprofen and aspirin to treat pain, and that opioid treatment for short-term pain last for three days, and rarely longer than seven. That is far less than current practice, in which patients are often given two weeks’ or a month’s worth of pills.They call for patients to be urine tested before getting prescriptions and for doctors to check prescription tracking systems to make sure patients are not secretly getting medicine somewhere else. They do not apply to prescriptions for patients receiving cancer or end-of-life treatment, or to patients who have had surgery. -See the full New York Times article.
Through Music, Memories Return Medscape Editor's Note: In 2014, a documentary called Alive Inside premiered at the Sundance Film Festival and picked up the audience award for best documentary. The film explores the idea that music can help reawaken memories and emotions in dementia patients and features the work of social worker Dan Cohen, MSW, whose nonprofit organization Music & Memory has improved the quality of life of thousands of patients through a very simple approach: giving them an iPod. Medscape recently spoke with Cohen about his rapidly growing initiative and about the therapeutic potential of personalized music in patients suffering from dementia. Medscape: How can music help patients with dementia and other cognitive problems? Mr Cohen: Music has multiple benefits. People with dementia who have lost their short-term memory often retain their long-term memory, especially for music. If you play music from someone's youth that holds personal meaning, it will help them stay connected with themselves and be more alive, alert, communicative, social, attentive, and more engaged. There is abundant research focus on music's ability to reduce blood pressure, improve mood, enhance sleep, as well as reduce agitation and anxiety. Research has also shown that it reduces behavioral and psychological symptoms of dementia. Then there is research around how music helps reduce pain, as described by an article from the Journal of Advanced Nursing in the 1990s. Music also helps to facilitate occupational therapy, physical therapy, and speech therapy. Music, speech, and movement are all interconnected in the brain. People fail rehabilitation because they're not getting up and walking. I remember this one gentleman who was not walking; he was given James Brown, and within a week he was walking 100 yards. There is no guarantee that music will generate hoped-for outcomes. Everyone is different. But the music that moves you now will probably move you the same regardless of cognitive impairment later in life. If you are unable to communicate what music you love, and no one else knows, you might end up listening to music you don't like. That's why people are beginning to integrate their list of favorites into their advance directives. Medscape: Alive Inside portrays pretty striking results with music interventions in dementia, but are there supporting data out there too? Have people run studies? Mr Cohen: Currently five Music & Memory-related studies are underway at four University of Wisconsin campuses. If you go to the New York State Department of Health website to the Electronic Dementia Guide for Excellence (EDGE), they recommend that all 650 nursing homes in New York State use individualized music to reduce agitation. It's been up for 10 years, and basically nobody has paid any attention to it. There is no money behind it and no requirement to do it. But the recommendation is based on the evidence-based research from Linda Gerdner, RN, PhD, who in the 1990s did what is considered excellent research. The foundational research is there. When music is playing, people are more likely to be reminiscing. People avoid visiting someone with Alzheimer disease even if they are at home. Family and friends stop visiting. If that person goes from their home to an assisted living facility or nursing home, it is no fault of the facility itself, but people think that somebody else is taking care of them, and they don't need to visit. That's a recipe for decline. Unfortunately, time-and-motion studies indicate that 90% of a resident's time is spent idle. Combine this with the fact that half of the people in nursing homes never—ever—get a visitor, and that makes for a bad combination even if your physical status is stable. It's a recipe for decline. Why live when nobody is visiting, and you have no meaningful relationships with anyone around you? We want to transform long-term care. How many of your readers are looking forward to going to long-term care? It's unlikely any would. Why is that? There are countries where people do look forward to it. What do we need to do? We need to make places that people enjoy being in where they will still have relationships and have a life. Music is one way to do this. Medscape: Practically speaking, how do you develop playlists for individuals? Mr Cohen: If we can, we work with individuals to compile their personalized playlist. But if they're unable to recall what music they enjoyed or meant something to them, then we'll work with the family. We'll ask, "Did they play an instrument when they were young?" "Did they sing in a choir or a chorus?" "Did they like Broadway musicals or religious music?" We'll ask if they have any old LPs sitting in a closet somewhere and what their wedding or high school prom song was. All of these kinds of questions help us figure this out. Aged care homes typically assume older patients want to listen to a popular music genre from their youth, such as big band. But unless that music holds personal meaning, perhaps associated to their senior prom, wedding song, or hanging with friends, it will probably just register as background noise. That's why we say that everybody should have their elders create a playlist. We should have all of our playlists in place. Neuroscientists say that this stuff works. We should help others in the family get their playlist together so that when they enter the healthcare system at any point—they go to the hospital, they go to hospice, wherever they go—their music goes with them and will help transform their experience. -See the full Medscape article.
|