|
MGH Community News |
|
MGH Community News |
| October 2019 | Volume 23 • Issue 10 |
Highlights
Sections Social Service staff may direct resource questions to the Community Resource Center, Hannah Perry, 617-726-8182. Questions, comments about the newsletter? Contact Ellen Forman, 617-726-5807. |
Court Imposes Nationwide Injunction on Trump Public Charge Changes In three rulings, federal judges in New York, California and Washington State issued injunctions temporarily blocking the “public charge” rule, which would impose serious impediments to legal residency for those who use benefits such as Medicaid or those deemed likely to use them in the future. The rule, widely seen as an attempt to keep out immigrants who are poor or in need of help, was one of the Trump administration’s signature immigration policies — and it ran into a legal brick wall in three corners of the country on a single day. While Trump’s legal setbacks add to several recent immigration initiatives blocked by the courts, the Trump administration has nonetheless been able to roll out policies that restrict asylum, tighten requirements for skilled-work visas and slash the number of refugees the country will accept. But the public charge regulations will not go into effect as quickly as the Trump administration desired. Two of the judges on issued nationwide injunctions on enacting the policy, while the judge in California limited her ruling to the nine western states within the Ninth Circuit. The public charge regulation had been roundly condemned by immigrant advocacy groups and the medical establishment, which argued that the rule would discourage immigrants from seeking government assistance when they may need help buying food or seeing a doctor.
Standards for public assistance were “never intended to exclude working-class immigrants from developing countries,” said Charles Wheeler, a director of the Catholic Legal Immigration Network, one of the plaintiffs in the case. “This ruling confirms that the American dream remains open to them.”
New handout: Public Charge Update: What Advocates Need to Know Now, October 17, 2019, from Protecting Immigrant Families. |
|
DHS clarified that the effective date of the final rule is postponed until there is a final resolution in the cases. The federal district court in New York also made it clear that the rule will not take effect until the injunctions are overturned. Under policy guidance from 1999 which remains in effect today for immigrants with applications processed inside the U.S., the use of health, nutrition and housing programs can NOT be considered in the public charge determination. -See the full New York Times article. Additional material from email statement from Madison Allen, Clasp, October 21, 2019.
El Salvador Temporary Protected Status Extended The Trump administration is extending protections from deportation to more than 200,000 Salvadoran citizens living and working in the United States in an announcement made Monday. Under the program called Temporary Protected Status — usually reserved to help foreign nationals from countries embroiled in wars or facing natural disasters — thousands of Salvadorans were allowed to stay in the U.S. following earthquakes in 2001. "The Trump Administration is extending the validity of work permits for El Salvadorans with Temporary Protected Status (TPS) through January 4, 2021," read a statement issued by the U.S. Department of Homeland Security.
The move apparently reverses a decision made in 2018 to end TPS for Salvadorans. The Trump administration also has tried to end TPS for people from Sudan, Haiti, and Nicaragua, among others. A federal judge has blocked the administration after a lawsuit was brought by the American Civil Liberties Union. Last month, the U.S. and El Salvador announced another agreement to stem the tide of migrants trying to reach the U.S. by sending asylum seekers to El Salvador. At the time, it was not clear that El Salvador's cooperation on asylum would be linked to any other bilateral issue, such as the status of Salvadoran TPS holders in the U.S. -See the full NPR story.
Massachusetts Senate Passes Bill to Create Registry of Caregivers Who Abuse People with Disabilities This month, the Massachusetts Senate unanimously passed a bill, S.2367, that would create a registry of care providers who have had an allegation of abuse of a person with an intellectual or developmental disability substantiated against them. Abuse is defined as an act that results in serious emotional or physical injury. The registry would be confidential, shared only with potential employers, who would be required to check the registry before hiring someone. DDS or any state-licensed care provider could not hire anyone on the registry. The bill would establish an appeals process for a worker who is put on the registry, and a person could petition to have their name removed from the registry after five years. If it becomes law, it would take effect Nov. 2, 2020. According to the bill’s sponsors, 26 states have registries to track individuals who abuse people with disabilities, based on agency investigations rather than criminal convictions. Moore said the bill is important because today, as long as a person is not convicted of abuse in court, there is no way for an employer to know that someone they hired has a record of abusing a client. Statistically, abuse of people with disabilities is rarely charged in court. According to the Disabled Persons Protection Commission’s annual report, in fiscal 2016 and 2017, around 1,500 cases each year of alleged abuse of people with disabilities were sent to a Massachusetts district attorney. But only around 100 cases each year resulted in criminal charges. “As long as there’s no database or no record of this, the person can go from one provider to another, subjecting people to multiple instances of abuse,” Moore said. Those who work with people with disabilities say there are many reasons a case might not go to trial. Victims may not be verbal, or their memories may be unreliable by the time something is reported. They may not want the public attention or the stress that comes with having to testify. They may face pressure from their abuser, or someone in power at an agency where they receive services, not to testify. “In the court system, our people are going to be at a disadvantage,” said Leo Sarkissian, executive director of the Arc of Massachusetts, which advocates for people with disabilities and has been pushing for the bill. Sarkissian said having a registry would set up a way for an abuser to be identified through a civil process and kept from harming others. House Speaker Robert DeLeo, D-Winthrop, declined to say this week whether the House will consider the bill this legislative session. DeLeo said he will talk to the relevant committee chairs. -See the full Mass Live article.
State Suspends License of Worcester Funeral Director Peter Stefan Known for Burying the Poor Worcester funeral director Peter Stefan, known for burying the poor and unwanted, has had his license suspended by the state. When reached by phone Wednesday morning, Stefan said a state inspector visited his funeral home — Graham Putnam & Mahoney — on Friday afternoon and suspended his license, citing an “imminent danger.” But Stefan, who has been taking abandoned bodies for years, denied the allegations, calling the situation a setup by the state. As reported last month (Unclaimed Bodies Languish While Mortician, Worcester Spar on Cremation Procedure), Stefan first caught the attention of officials in August when a backlog of bodies began to create an odor in his funeral home. He said he collected the group of relativeless-bodies from UMass Memorial Medical Center back in May. Some, he said, had been dead for seven or eight months. Stefan said the situation got out of control after the city failed to sign cremation forms for months. The longtime funeral director spoke before the City Council Tuesday night to raise concerns about a different topic -- the state’s policies surrounding payments for burying to poor. Stefan told the Council that the state owes him more than $100,000 for burying poor veterans. He said something needs to be done to alleviate the problem, saying Massachusetts should create an estate recovery unit to locate veterans’ assets. “All across the state, I hear the same problems,” he said.
Stefan said he has been taking bodies of the poor and unwanted for nearly 20 years -- usually at a loss. -See the full Mass Live article.
Adult Foster Care- The Adult Family Care Program Adult Family Care, Somerville‐Cambridge Elder Services’ Adult Foster Care program, helps people receive care at home, by supporting family or friend caregivers who live with the person receiving care. The program serves MassHealth eligible people who cannot live alone due to a medical diagnosis. Caregivers through Adult Family Care receive a tax-free stipend, ongoing training, and two weeks paid respite annually. Adult Family Care provides:
Eligibility Requirements:
Adult Family Care serves much of the Greater Boston Area. More information or to make a referral. -Thanks to Nathan Lamb, Somerville-Cambridge Elder Services, for this article.
Crossroads Resource Center Celebrates Grand Opening Two Charlestown health centers have come together to collaborate on a drop-in resource center, particularly for those struggling with addiction and other such issues. NEW Charlestown and the Charlestown MGH Health Center have collaborated on opening the Crossroads Resource Center within the NEW Health Center in Hayes Square. The space has been carved out of what was a conference room in the Health Center, and offers a five-day drop-in center that is staffed by personnel from both health centers. Resource Specialist Gina Cardone said the Center offers recovery coaches, including Shannon White from MGH and Lorraine Fitzgerald from NEW Charlestown. Additionally, it offers people who are patients or just community members a place to relax, to get help with things like job applications, to use computers or to simply get a cup of hot coffee while having a conversation. The idea was born by the Centers’ two medical directors – MGH’s Jim Morrill and NEW Health’s Anne Murray Chiriboga – who felt that the Town needed a Center for people to come to. Space was available at NEW Charlestown in the underutilized conference room, and they figured – why not work together? Crossroads is is staffed with those offering recovery resources, and other resources like social service and housing matters. They have coffee, snacks and computer access as well. One thing that has been important, both doctors said, was to let the clients and Recovery Coaches define what the space would be. That means it is constantly evolving with the needs of those using it – but always with a strong recovery theme to it. The Crossroads Resource Center is open weekdays, Monday through Friday, 12:30-3:30 p.m., 15 Tufts St, Charlestown. -See the full Charlestown Bridge article. -Thanks to Marie Elena Gioiella for sharing this resource.
Jack & Jill Foundation- Creating WOW! Experiences for Families with a Parent with Late-Stage Cancer The Jack & Jill Late Stage Cancer Foundation (JAJF) helps kids under 18 who are facing the imminent loss of their young Moms and Dads to cancer. While the children do not have cancer physically, their worlds have been turned upside down by their parent’s disease. When mom or dad is diagnosed with late stage cancer, children are faced with the reality the rest of their lives will never be quite the same. JAJF understands the stress cancer places upon the family structure and provides families a chance to spend quality, positive (FUN) time together in the face of these hardships and uncertainties… as prescribed by their Oncologist. JAJF partners with a variety of entertainment, transportation and hospitality organization to tailor once-in-a-lifetime experiences for these families. Experiences include resorts, ballgames, concerts, amusement parks, dude ranches, festivals, helicopter rides and more. There is no financial need criteria. For more information see JAJF FAQs. Patients must be referred by their Oncologist. Learn more about the referral process at: https://jajf.org/oncologists/referral-process/. To refer a family, please download and complete the Oncology Referral Form and return to (404) 920-2139. -Thanks to Sandy McLaughlin for sharing this resource.
Free Yoga, Meditation, Pilates or Mindfulness Classes for Cancer Patients and Survivors Boston Cancer Support seasonally sponsors 4 wellness grants open to Massachusetts residents. Recipients must be either a cancer survivor, or currently in treatment (with physician approval). Apply for one of four grant opportunities below. The grants are for one of the following:
The current grant cycle is open through December 15th. Recipients are announced on January 1st: Learn more and apply here. For more information or to apply: https://www.bostoncancersupport.org/randi-friedman-wellness-grants/ -Adapted from emailed statement from Boston Cancer Support, October 10, 2019.
Perkins Library for Free and Accessible Resources for People with Disabilities The Perkins Library provides accessible reading material to Massachusetts residents. Each state has their own National Library Service library. The Perkins Library offers a variety services to eligible patrons, both adults and children, including of course a growing collection of physical cartridge and cloud-based talking books, braille and large print books, all available through postage-free checkout and delivery. They also offer a same-day newspaper and magazine telephone service called NEWSLINE, an audio described Blu-ray and DVD library, museum passes, book clubs, and catalogues such as the Talking Book Topics the Braille Book review. To search their entire catalog please visit https://webopac.klas.com/ma1aopac. To get a better sense of how audio description works, the following web address links to an audio-described trailer of the movie War Horse (DVD 1005).
See the Application for Library Services, or read more about their services: Individual Patron Information Sheet. See the Library website at www.PerkinsLibrary.org and the National Library Service website at www.loc.gov/nls for more information.
-Thanks to Zary Amirhosseini and Erin Fragola, Library Outreach Coordinator, Perkins Library, for their help with this article.
ConnectorCare Open Enrollment 2020: November 1, 2019 to January 23, 2020 In 2019 ConnectorCare was an important source of affordable health insurance for over 220,000 Massachusetts residents with incomes of 300% of poverty or less. The Health Connector is able to automatically renew about 69% of 2019 ConnectorCare members into continued ConnectorCare coverage for 2020. About 26% will be losing their subsidies for 2020; however, in most cases the reason is missing income information, and many can retain 2020 ConnectorCare coverage by just updating their income. Open enrollment is also an important time for ConnectorCare members to compare plans and make sure they are enrolled in the best plan for them. It is also an opportunity for those who were found eligible in 2019 but missed the enrollment deadline to update their information and, if still qualified, sign up for ConnectorCare for 2020. More information about Open Enrollment for 2020 including links to resources for individual assistance are posted here: https://www.masslegalservices.org/content/open-enrollment-2020-connectorcare Note: those living in most other states must enroll in their state by December 15 unless they qualify for subsidies or have a qualifying life event that allows them to enroll outside of Open Enrollment. -From Health Update October 2019, Vicky Pulos, Mass Law Reform Institute, October 21, 2019.
MassHealth: Affidavits for Proof of Zero Income, Massachusetts Residency, and Incarceration Status MassHealth requires applicants and members to verify certain eligibility factors including, but not limited to, income and residency. If MassHealth is unable to verify a certain eligibility factor through data matches, additional documentation is required. MassHealth has created three affidavits as a way to verify zero income, Massachusetts residency, and incarceration status for applicants and members who have no other way to verify these eligibility factors. Using the New Forms These forms may be offered to applicants and members who either walk in or call for assistance and have no other way to verify these eligibility factors. These forms are effective immediately. An affidavit does not have to be on one of these forms to be acceptable, as long as the necessary content and signature(s) are present. As with all factors that may be verified with an affidavit, whether on one of these forms or in another format, it does not have to be notarized. As long as the statement or affidavit includes all of the necessary information and signatures, the eligibility factor should be verified. Submitting the Form Forms can be submitted to the Health Insurance Processing Center by mail or fax, or to any of the MassHealth Enrollment Centers (MECs), or Health Connector walk-in centers in person. All of the contact information is listed on the affidavit. Obtaining the Form Forms can be found on the Health Connector web site at: www.mahealthconnector.org/verification-documents and on the MassHealth website at www.mass.gov/service-details/masshealth-member-forms. -Adapted from MassHealth Acute Inpatient Hospital Bulletin 172, October 2019.
As Promised Help for DCF Lags, Top Lawmaker Launches Unusual Oversight Abused and neglected children awaiting foster placement are more likely to be playing in licensed day care centers, rather than crawling around grimy office floors at the Department of Children and Families. And frazzled families now have more social workers to help them navigate the department’s byzantine foster system. But nearly five months after Governor Charlie Baker’s administration pledged to upgrade the state’s troubled foster care system, some serious problems remain. Social workers are still scrambling many nights to find children emergency foster placements, relying on a chaotic, often paper-based system for tracking kids. The Baker administration said in May that a new after-hours hot line database to track open foster homes in real time would be up and running by Nov. 1. But officials said this month it won’t be operational till January. Meanwhile, an online service for foster families to communicate with each other and exchange vital information about the kids they’re caring for has had a rocky start. Families are also still waiting for more in-depth training on how to care for severely traumatized children. And, crucially, foster children still face long waits for mental health therapy, which has been one of foster parents’ top concerns. The state held eight public hearings over the summer, asking residents their thoughts on how to improve the state’s behavioral health system for everyone, but it has not yet announced next steps. “The Department of Children and Families is working to implement all of the reforms originally announced in collaboration with SEIU Local 509 [the workers’ union] in May,” the agency said in a statement last week. House Speaker Robert A. DeLeo last Wednesday directed the House Ways and Means committee vice chair, Denise Garlick, a nurse who has led several health-related legislative committees, to serve as his point-person on improving the foster care system, as the Legislature ramps up its oversight of DCF. In an interview, Garlick, a Democrat from Needham, said she intends to seek out colleagues, families, and community leaders as lawmakers develop DCF-related legislation and the state budget in the coming months. She said past legislative work she’s done related to grandparents raising children and families roiled by opioids — both prevalent in the foster care system — would inform her thinking. Mary McGeown, president of the Massachusetts Society for the Prevention of Cruelty to Children, said Garlick’s appointment is critical because it means a legislative point person will be looking at the problems comprehensively — and will have the speaker’s ear. “You don’t want to see the attention of the administration ebb and flow by crisis,” McGeown said. -See the full Boston Globe article.
Foster Children, Parents, Push for Outside Review of DCF Cases Morriah Bosco spent 18 years in the foster care system. She was moved 40 times. Bosco said the Department of Children and Families wrote on her placement plan that her goal was reunifying with kin — but no one actually looked for a family member to take her in. She was never given a permanent placement or a plan to help her age out of the system. “I confronted a supervisor and she said ‘What are we supposed to put down? There’s no plan for you,’” Bosco said. No one, she said, oversaw DCF. While federal law requires every foster care case be reviewed every six months, Bosco said she once went 18 months in a restrictive setting without a review. Bosco was among the former foster children, parents and advocates who testified at a hearing of the Joint Committee on Children, Families and Persons with Disabilities this month about the need for an independent office to oversee foster care reviews. The bill, H.112/S.29, sponsored by Rep. Tricia Farley-Bouvier, D-Pittsfield, Rep. Aaron Vega, D-Holyoke, and Sen. Jo Comerford, D-Northampton, would establish an independent Massachusetts foster care review office. The office would be responsible for regularly reviewing every case in which a child is removed from their home, ensuring the child has a plan for permanency, and collecting information from the reviews to inform DCF policy. These reviews are mandated by federal law, and today, they are conducted by a special unit within DCF. But advocates for children have long complained that these reviews are inadequate and done in a pro forma way that does not provide sufficient oversight. Northwestern District Attorney David Sullivan, who used to work for an adoption agency that placed adolescents, said cases often linger in the system for too long “with the workload of DCF case workers, schedules of attorneys, and rights of parents taking precedence over children.” Sullivan said DCF workers, concerned with immediate challenges, often do not have the capacity to reflect on a child’s long-term well-being. Sullivan said DCF, like any agency, has blind spots about its own performance. “When asked about foster care reviews, two retired DCF workers referred to these reviews a ‘a joke,’” Sullivan said in testimony submitted to the committee. Farley-Bouvier said having an agency that polices itself is not good for children or for the agency, which lacks data on what is working and what is not. She noted that the agency, in reviews, rarely disagrees with itself. “I’m sorry to say that often times within DCF we take bad situations and we make them worse,” Farley-Bouvier said. Some states, like Nebraska, already have reviews conducted by an outside agency. Farley-Bouvier said the changes DCF is implementing “are just nibbling around the edges.” “It’s time we make bold changes when it comes to child welfare,” Farley-Bouvier said. “I believe this idea of taking the review of foster care outside the agency will be able to do just that.” -See the full Mass Live article.
Parents Fighting for Custody of Their Kids Thwarted by DCF Office Moves In the summer of 2018, the Department of Children and Families moved its bustling downtown Lowell field office to a remote office park in Chelmsford. In July, it relocated its downtown Malden office from a public-transit-friendly location to an office park in Wakefield harder to reach by bus or the subway. Now, DCF is making plans to move its busy Cambridge office to suburban Burlington. Using words like “disastrous” and “bleak,” lawyers for hundreds of struggling parents who have lost custody of their children say the office relocations have created significant transportation hurdles for many families. Parents, many of whom don’t have cars, must now trek to these hard-to-reach offices for state-monitored visits with their children. Often they are struggling with addiction while trying to repair fragile family bonds and regain custody. The lawyers say the agency that is supposed to be devoted to building stronger families is instead creating obstacles that tear them apart. “Our clients are disproportionately poor and disproportionately dependent on public transit or the kindness of friends,” said Michael Dsida, deputy chief counsel at the state public defender agency, the Committee for Public Counsel Services. “When [public transit] is taken away or significantly scaled back, it makes it harder for them to see their children and their children to see them.” Spokespeople for DCF and the state’s Division of Capital Asset Management and Maintenance (DCAMM), the agency that procures government offices, declined to say whether the agencies seek public input about transportation needs when securing new DCF offices. DCF said that it’s also trying to move some family meetings into more inviting spaces. Since 2017, it said it has hired 107 social worker technicians, and plans to hire 29 more by July, to supervise meetings for parents allowed to visit their children in family-friendly places, such as parks, libraries, or relatives’ homes. But lawyers say visits outside DCF offices are not often granted, despite a low risk of parents absconding with or harming a child. And yet, lawyers say, these outside visits are critical for adding a sense of normalcy to a fraught gathering. In a blunt letter to DCF, the state public defender’s agency said the Lowell relocation to Chelmsford “has been a disastrous move for the families that DCF serves.” The letter describes significant gaps in the schedule for the single bus line that stops close to the new office park in Chelmsford. And parents are expected to play with their children in grim, windowless rooms. “Visits are bleak at the DCF facility,” it says. “There is nothing to engage a family near the Chelmsford office, no outdoor playground, no local fast food chain, no urban street to stroll along and window shop.” The vast majority of children removed from their parents by DCF and placed in foster care ultimately are reunited. That, said Dsida, makes it all the more imperative for the agency to make visits accessible and substantive, not relegated to stark rooms in hard-to-reach office parks. “It’s incumbent on DCF to make [reunification] happen smoothly and quickly,” he said, “and with as little trauma as possible.” -See the full Boston Globe article.
Trump Administration’s Plan to Require Immigrants Show Health Insurance Earlier this month, President Trump issued a proclamation that immigrants seeking visas while abroad will be denied admission to the U.S. if they cannot show that they will be covered by certain types of unsubsidized health insurance, Medicare, or TRICARE within 30 days of entering or have financial resources to pay for “reasonably foreseeable medical expenses.” The policy is set to take effect November 3, 2019, and will not be applied retroactively to individuals issued visas prior to that date. Certain other categories of immigrants are also exempt including legal permanent residents (LPRs or green card holders) returning after a long absence and parents of adult U.S. citizens who can demonstrate to the consular officer’s satisfaction that their health care will not impose a substantial burden on the U.S. health care system. This restriction, which would operate independently of the “public charge” determination, represents the latest move by the Trump administration to curtail immigration by people who cannot pass a wealth test. To whom does the proclamation apply? The proclamation would deny entry into the U.S. to people seeking family-based immigrant visas (and some others) if they are unable to show that they will be covered by certain insurance products within 30 days after entering the country or have the financial resources to pay out-of-pocket for “reasonably foreseeable medical expenses.” The proclamation would apply to people seeking immigrant visas abroad, including: spouses of U.S. citizens and lawful permanent residents (LPRs); children of LPRs who are 18-21 years old; children under 18 if travelling with a parent who is also immigrating; adult sons and daughters of U.S. citizens and LPRs; people with diversity visas or employment-based immigrant visas; and some religious workers. It would also apply to parents of U.S. citizens who cannot show that their health care will not impose a substantial burden on the U.S. health care system. Which forms of health insurance are “approved” under the proclamation? “Approved” health insurance under the proclamation includes:
Medicaid is acceptable for children age 18 and younger, but subsidized ACA plans are not acceptable for either adults or children. Who is exempt from the proclamation’s requirements? Certain categories of immigrants are exempt from the proclamation’s requirements, including:
The proclamation further states that it should not be construed to affect any individual’s eligibility for asylum, refugee status, withholding of removal, or protection under the Convention Against Torture. Analysis The Migration Policy Institute recently crunched the numbers and posted an excellent Twitter thread, noting that the proclamation could exclude 2/3 of future immigrants. At The Washington Post, Catherine Rampell called the proclamation a “presidential twofer,” simultaneously sabotaging our health-care and immigration systems. Protecting Immigrant Families has developed the following talking points:
Read the National Immigration Law Center’s summary. -Sources and for more information: National Immigration Law Center’s summary; Medicare Dental & Other Improvements Move Forward, Justice in Aging, October 18, 2019 and Trump’s Proclamation Requiring Immigrants to Have Health Insurance, Madison Allen, CLASP, October 08, 2019.
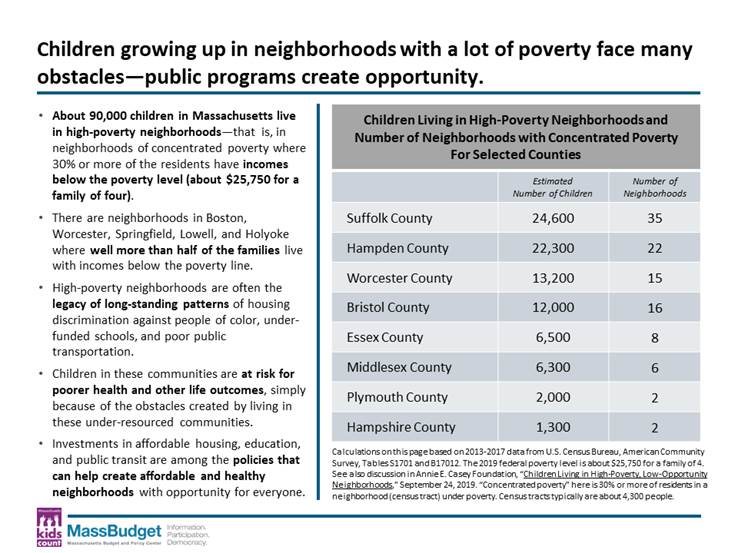
90,000 Kids in Massachusetts Live in Concentrated Poverty Did you know that more than 1 in 16 children live in concentrated poverty in the Commonwealth? Using recent data from the U.S. Census Bureau and the Annie E. Casey Foundation's data snapshot, MassBudget examined how concentrated poverty has affected children across the state despite a long period of national economic expansion. In Massachusetts, living in high-poverty neighborhoods affects six percent of all children, and these neighborhoods are mostly in Gateway Cities and the City of Boston. "Growing up in high-poverty neighborhoods has long-term impacts on our kids," said Marie-Frances Rivera, MassBudget's President. "All children and families deserve quality education, housing and access to opportunity. Investing in solutions that uplift children in poverty will create the change needed for everyone in the Commonwealth to thrive." Growing up in a community of concentrated poverty - that is, a neighborhood where 30 percent or more of the population is living in poverty - is one of the greatest risks to child development. Alarmingly, more than 8.5 million children live in these settings. That's nearly 12 percent of all children in the United States. Children in high-poverty neighborhoods tend to lack access to healthy food and quality medical care and they often face greater exposure to environmental hazards, such as poor air quality, and toxins such as lead. Financial hardships can also cause chronic stress linked to diabetes, heart disease and stroke. And when these children grow up, they are more likely to have lower incomes than children who have relocated away from communities of concentrated poverty. Children should be allowed to learn and grow no matter where they live or their socioeconomic status. Policies at the community and state level that can have a significant impact on the lives of children in struggling families include:
Interested in learning how you can help combat child poverty? View the snapshot here and join the conversation online @MassBudget. -From Concentrated Poverty Affects 90,000 Massachusetts Children Economic Growth Doesn't Reach All Neighborhoods in the Commonwealth, Reginauld Williams, MassBudget, October 03, 2019.
Number of Uninsured Children Rises for Second Year, Tops 4 Million The number of uninsured children in the U.S. increased for the second year in a row and now tops four million, the highest numbers since ObamaCare became law, according to a new report released Wednesday. According to the Georgetown University Center for Children and Families, the number of uninsured children increased by more than 400,000 between 2016 and 2018. The report found that increase has wiped out a large share of the coverage gains made since the enactment of the health law in 2014, and is due in large part to policies championed by the Trump administration and Republicans in Congress. According to researchers, ObamaCare helped more children obtain health coverage. But beginning in 2017, the number of uninsured children began to rise. The report specifically cited the confusion surrounding the administration’s failed attempt to repeal ObamaCare, the successful elimination of the law’s individual mandate, and a months-long delay in funding the Children’s Health Insurance Program (CHIP). In addition, the report cited the Trump administration’s decision to dramatically cut ObamaCare outreach and enrollment grants, while also shortening the open enrollment period. “At a time when families need more help navigating the confusing health coverage landscape, fewer resources are available for ObamaCare outreach and enrollment efforts as a result of cuts made by the administration in 2017,” the report said. Three-quarters of the children who lost coverage between 2016 and 2018 live in GOP-led states that have not expanded Medicaid. The uninsured rate for children in those states increased at three times the rate as children in expansion states. The majority of uninsured children are eligible for Medicaid or CHIP but are not currently enrolled. Researchers also pointed to President Trump’s crackdown on immigration as a reason why the number of uninsured kids is rising. Several policies targeting immigrant communities, like the administration's "public charge" rule, are likely deterring parents from enrolling their eligible children in Medicaid or CHIP, despite the fact that most of these children are U.S. citizens. -See the full The Hill article.
|
 All books and magazines are digitized and are either saved on special USB thumb drives called “cartridges” which can be mailed through the US postal service or downloaded to smart devices through the online database. They loan out the machines to play the cartridges, on long term loan. The cartridges are then returned when patrons have finished with them. Headphones are also available at no cost upon request.
All books and magazines are digitized and are either saved on special USB thumb drives called “cartridges” which can be mailed through the US postal service or downloaded to smart devices through the online database. They loan out the machines to play the cartridges, on long term loan. The cartridges are then returned when patrons have finished with them. Headphones are also available at no cost upon request.