|
MGH Community News |
|
MGH Community News |
| November 2023 | Volume 27 • Issue 11 |
Highlights
Sections Social Service staff may direct resource questions to the Community Resource Center, Hannah Perry, 617-726-8182. Questions, comments about the newsletter? Contact Ellen Forman, 617-726-5807. |
Winter Moratorium on Utility Shut-Offs Now in Effect - Not All Are Covered
The MA winter moratorium on heat-related utility shut-offs began on Wednesday November 15 and will last through at least March 15 (typically extended to April 1). State law and MA Department of Public Utilities (DPU) regulations prohibit termination of electric or gas service between Nov. 15 and Mar. 15, if the utility service provides heat OR is needed to operate the heating system, AND the customer has a financial hardship. Conversely, that means electric or gas service can be terminated if the customer does not have - and document - a financial hardship, or if that utility service is not involved in providing heat (for example, electric service to a rental unit can be terminated if the landlord has a central heating system because the tenant would still have heat). National Grid and Eversource have said they will be suspending disconnections of all residential heat customers, regardless of whether they are on the discount rate (coded as low-income) or not. Both will also suspend disconnections of discount rate electricaccounts (for those who do not have electric heat; but electricity is typically needed to run heating systems, thermostats, etc.) For those not on the utility’s discount rate, Eversource specified that they allow self-attestation of financial hardship in the winter to get on the discount rate, to either stop a shutoff or get service restored (if terminated after November 15). Customers will just have to fill out a self-declared financial hardship form. - From [utility network] Updates: Winter terminations, Anna Kowanko, NCLC November 13, 2023 and Charlie Harak, NCLC, Nov 2, 2023.
Employees Can Now “Top Off” MA PFML A recent change regarding the MA Paid Family and Medical Leave (PFML) law affects both employers and employees. |
For applications filed on or after November 1, 2023, employees receiving PFML benefits may supplement (or “top off”) their PFML benefits with any available accrued paid leave (sick time, vacation, PTO, personal time, etc.). For employees who choose to supplement their PFML benefits in this way, the combined weekly sum of PFML benefits and employer-provided paid leave benefits cannot exceed the employee’s Individual Average Weekly Wage (IAWW). Employers will be responsible for monitoring and ensuring that the combined weekly sum of employer-provided paid leave benefits and PFML benefits does not exceed an employee’s IAWW. If the application is filed on or after November 1, 2023, applications filed retroactively for a leave that began before November 1, 2023, are eligible for topping off. Employers are also responsible for managing any payments made to an employee that exceed the employee’s IAWW. The Department of Family and Medical Leave (DFML) is not involved in the repayment process for top off overages. This process is solely the responsibility of the employer and the employee. Learn more at the PFML website, including information about 2024 maximum benefit amounts, employer contribution rates, and more. - From Vaccine Guidance; Equity Opportunity; PFML, MHA's WEEKLY WRAP-UP, November 10, 2023.
2024 Medicaid SSI, Spousal Impoverishment, and Medicare Savings Program Financial Eligibility Standards This month, the Centers for Medicare and Medicaid Services (CMS) published the updated 2024 Medicaid financial eligibility standards for Supplemental Security Income (SSI) and spousal impoverishment protections, as well as the resource limits for the Medicare Savings Programs (MSPs). As of January 1, 2024, the resource limits for three MSPs (QMB, SLMB, and QI) will be $9,430 (single) and $14,130 (married). In 2024, the 300% SSI income limit will be $2,829, while the SSI resource limit remains at $2,000 for an individual. The bulletin also provides the 2024 minimum and maximum maintenance needs allowance, community spouse housing allowance, community spouse resource standards, and home equity limits. This bulletin and a chart summarizing the SSI and Spousal Impoverishment Standards is posted on Medicaid.gov. - From From DC: Medicaid Eligibility Standards, HHS Report on Older Adult Homelessness, and more, Justice in Aging, Friday, November 17, 2023.
4 More Free COVID tests Will be Available to Each Household Ahead of the Holidays Ahead of the approaching holidays and a potential rise in cases this winter, the government is once again allowing households to order a fresh wave of four COVID-19 tests for free online. The website, covidtests.gov, remains one of the last remaining ways Americans can secure free at-home rapid test after the end of the public health emergency last spring ended the requirement for insurance companies to cover eight tests per month. Over the past three years, the return of winter has also brought a resurgence of COVID-19. According to modeling data from the Centers for Disease Control and Prevention, health officials are anticipating a similar number of hospitalizations this year as they saw last year, which topped nearly 45,000 per week at its peak. The test ordering site relaunched last month, offering four tests per household, and will now offer an additional four tests per household for anyone who has already ordered -- or eight tests per household for anyone who hasn't placed an order yet this fall. - See the full ABC News story.
88,000 people dropped from MassHealth in October, Most for Lack of Information About 88,000 more people lost MassHealth coverage in October, the largest monthly decline yet in the year-long effort to reassess eligibility for 2.4 million members. Most of those losing coverage to date have been dumped for procedural reasons. Through the first seven months of the process in Massachusetts, 46% of people kicked off MassHealth lost their coverage because officials confirmed they no longer qualify. Another 52% lost coverage because state workers did not have enough information to assess eligibility, state officials said. Data published by state health and human services officials on Tuesday show that the state's combined Medicaid and Children's Health Insurance Program rolls have dropped by a cumulative 112,000, or 4.67%, since April. Officials said they still believe the number of disenrollments will nearly triple over the five remaining months in the federally required redetermination campaign, forecasting a sizable jump this winter following open enrollment at the Massachusetts Health Connector. The Connector, a state-run insurance marketplace that also offers some subsidized coverage options, has seen a significant uptick in interest as the redetermination process unfolds. MassHealth officials said Tuesday that enrollment through the Connector has grown by 38,000 since April, suggesting "a large portion of the individuals who have lost MassHealth eligibility are able to obtain affordable coverage" with policies offered through the insurance clearinghouse. All 50 states are undergoing similar efforts to reassess eligibility for Medicaid plans. The federal government prohibited removing people from Medicaid during the COVID-19 pandemic in an attempt to keep Americans covered, but that requirement ended this year. States must now figure out who still qualifies for publicly funded health insurance and who needs to be removed from the programs. About 22,000 people newly enrolled in MassHealth in October, a roughly average amount that partially offset the 88,000 departures, according to the data. Healey administration officials projected at the start of the campaign that it would lead to a net reduction in MassHealth enrollment of 300,000 to 400,000 members, freeing up $1.9 billion in funds that are being used elsewhere in this year's state budget. Assistant Secretary for MassHealth Mike Levine said Tuesday those annual estimates still hold. The share of disenrollment for procedural reasons has been increasing in recent months, and Levine said he is grappling with how to interpret the data because it provides a single count for two distinct types of people: those who intentionally ignore contact from MassHealth because they already know they are ineligible, and those who might still qualify but fall through the cracks or cannot be reached. Some Bay Staters, Levine said, joined MassHealth early in the pandemic, and their life circumstances have changed significantly since then — for example, they might have gotten a new, well-paying job with employer-sponsored insurance. And because federal requirements prohibited states from disenrolling people before the redetermination campaign kicked off, those people are still on the rolls. They wouldn't be automatically renewed in MassHealth because the state can see from a tax return or a wage report they earn well above the required income threshold. However, when MassHealth follows up with a "blue envelope" confirming their personal details, such members often do not reply, forcing them to get counted as terminated for procedural reasons. On the flip side are MassHealth members who are likely still eligible, but for whom income information is not available in an existing public database, meaning they can't be automatically renewed. If those people fail to reply to a blue envelope, they, too, get counted as terminated for procedural reasons. One data point Massachusetts officials are watching closely as a way to understand the dynamic is the number of people who rejoin MassHealth after leaving, which totaled about 11,000 in October. Bay Staters who returned to MassHealth within three months of departing "were probably always eligible, then missed the blue envelope, or something happened that was more procedural," Levine said. "[That is] exactly the kind of thing that we've organized ourselves around trying to reduce as much as possible," he said. - See the full WBUR article.
Those Whose SSI was Wrongly Reduced or Terminated During the Early Pandemic Will be Repaid A court has approved a settlement in Campos v. Kijakazi, that will benefit more than two million Supplemental Security Income (SSI) recipients who incurred overpayments during the COVID-19 National Emergency due to Social Security Administration (SSA) offices being closed or inaccessible. Background The Social Security Administration wrongfully reduced and discontinued SSI benefits for thousands of people during the pandemic while the agency’s offices were closed, leaving the plaintiffs with no way to engage with the agency to get their benefits reinstated. In March 2020, SSA closed its field offices in response to the COVID 19 pandemic. The agency had no remote work plan so at that time the agency stopped processing information from recipients about their finances and stopped sending notices of benefit changes. Beginning in September 2020, agency workers begin working remotely and resumed sending notices of reduction and termination of benefits to thousands of people. With offices closed, it was extremely difficult, if not impossible, for recipients to resolve problems with those notices. The Social Security Administration issued an interim rule in August 2020, due to the national emergency, that was intended to create an easier process to waive certain overpayments during the early months of the pandemic. However, the agency didn’t inform people the no-fault streamlined waiver even existed, and the waiver only covered the first six months of this ongoing pandemic. If an individual did learn about the waiver, they still faced extreme barriers and difficulties reaching employees of the agency to resolve problems, especially for those without access to technology or the internet. Many people lost benefits or had them reduced. In some states, losing SSI benefits can also lead to losing Medicaid. The New York Legal Assistance Group, Justice in Aging, and the law firm Arnold & Porter filed a class action lawsuit on behalf of five SSI recipients challenging the agency’s unlawful practices. The Settlement: Waiver of March-September 2020 Manual SSI Overpayments with No Action Required by SSI Recipients
*SSA will not waive: Any such overpayments resulting from fraud or similar fault or involving misuse of benefits by a representative payee or that have already been reversed or waived. Where Applicable, Refunds of Funds Previously Paid with No Action Required by SSI Recipients
Administrative Guidance about COVID-19-Related Circumstances as Basis for Waiver By late February 2024, SSA will issue internal guidance reminding technicians how to adjudicate waiver requests, specifically directing them to consider COVID-19-related circumstances when making findings of fault for overpayments that arose during the COVID-19 National Emergency Period (March 2020-April 2023) including, for example:
Notice to SSI Recipients Assessed Overpayments for COVID-19 Emergency Period
More Information
- See the full posts from Justice in Aging Campos et al v. Kijakazi litigation and Campos et al v. Kijakazi Settlement Information for Advocates.
Head Start Staff Shortages Lead to Waitlists and Closures Recent staffing shortages at Head Start programs have forced centers across Massachusetts to cut slots for children, placing infants and toddlers on lengthy waitlists for its affordable care and educational opportunities. At least three centers — in Greenfield, Amherst and Boston — have shut down entirely. Head Start provides crucial services, like meals and early learning, to roughly 11,000 Massachusetts children from infancy to age 5. Children qualify for Head Start if they're in foster care, lack housing or their families meet federal poverty thresholds. Early education experts blame the worker shortage on low wages. According to Head Start, its teachers in Massachusetts make on average $39,000 a year — or half the average salary of a public K-12 teacher in the state. Head Start gets most of its money from federal funding: $180 million for its Massachusetts program last year. Massachusetts is one of several U.S. states that supplements those federal dollars, allocating another roughly $17.5 million for Head Start last year. Still, program directors argue state and federal funds have not kept up with rising operational expenses, like rent or utilities. And, the strained budgets, they say, make it difficult to pay teachers competitive wages. Some Head Start directors said they've resorted to permanently reducing classroom seats to cope with the staffing constraints and make room in their budgets for teacher pay bumps. Several directors said resizing allowed them to use the savings to boost teacher pay. - See the full WBUR story.
Mass. Attorney General Reaches $8M Settlement with Rent-A-Center Rent-A-Center, one of the nation’s largest rent-to-own companies, recently reached a $8.75 million settlement with the state’s attorney general’s office in order to resolve allegations the company violated Massachusetts law by routinely using unfair and deceptive practices against consumers. Massachusetts Attorney General Andrea Campbell announced Tuesday morning that the rental company agreed to pay the multi-million settlement as well as make significant changes in its business practices to follow the state’s consumer protection laws, including fair debt collection and repossession practices. Based in Plano, Texas, Rent-a-Center operates more than 40 retail locations in Massachusetts. Many are located in predominantly low-income communities and communities of color, according to Campbell’s office. The company was founded in 1973 and it specializes in renting furniture, appliances, electronics and computers to customers, according to its website. After an investigation by the Attorney General’s Office of Consumer Protection and Civil Rights Divisions, the office alleged that Rent-A-Center repeatedly used coercive and abusive conduct towards customers who missed or failed to make rental payments under rental contracts. In an effort to coerce consumers into making additional rental payments, the AG’s office found that the company regularly filed applications for criminal theft and larceny against consumers who failed to make payments. Even for customers who paid significant amounts of money to the rental company over multiple years before falling behind on payments, the AG’s office found that the company sought criminal charges. As part of the settlement agreement, the rental company will no longer continue its practice of filing criminal complaints against consumers for missing payments. The AG’s investigation also found that the rental company excessively called consumers’ homes, workplaces and personal phones in violation of the debt collection rules. The rule states that debt collection calls can only be made to consumers twice within a seven-day period. Consumers who believe they may have been subject to unfair and deceptive business practices may file a consumer complaint with the AG’s Office. - See the full MassLive article.
BMC offers Job Training to Patients to Join Their Workforce In early 2023, a group of leaders at Boston Medical Center sat down to discuss a big idea: What if we started a jobs training program for our patients so that they could get the skills to join our workforce? We called it the “BMC Healthcare Fellowship Program,” and while it was seemingly simple in its design, we knew we should start small to test its viability. In the spring, we began the pilot in the Family Medicine clinic at Boston Medical Center. The road map for recruiting fellows came from our Social Determinants of Health screener — a tool for every patient in primary care that screens for, among other things, food, job, and housing insecurity. While there are increasing calls for political leaders to create more jobs training and even an action report for future governors, few health care leaders are taking the economic mobility of their patients into their purview. This gap is understandable — the health care system is fragile; we have people leaving the field every day with high burnout rates, and health care workers are already tasked with so many administrative burdens. However, creating opportunities for job training and economic mobility is one of the best things health leaders can do for our patients’ health and, in the long run, for the well-being of our country. Health care leaders, payers, policymakers, and community members must come together to creatively tackle and build paths of economic mobility. For while the words of Mahatma Gandi, “it is health that is real wealth and not pieces of gold and silver,” still ring true, the data are now clear that health cannot be fully achieved without a baseline of wealth. - See the full Boston Globe opinion piece.
CMS Finalizes Rule Improving Medicare Dental Coverage for Cancer Patients The Centers for Medicare & Medicaid Services (CMS) has finalized the 2024 Physician Payment Schedule. The rule clarifies additional instances in which Medicare will pay for dental services that are integral to covered medical services, including services for head and neck cancer treatments, for the treatment of cancer prior to or during chemotherapy, and additional cancer therapies. Dental and Oral Health Services Historically, Medicare has paid for dental services in some clinical circumstances when dental services are inextricably linked to the clinical success of specific covered medical services. In last year’s PFS final rule, we codified that Medicare payment under Parts A and B could be made when dental services are furnished in either the inpatient or outpatient setting under particular kinds of circumstances. Among other provisions CMS finalized:
For CY 2024, we are building up on our efforts in the CY 24 PFS final rule and are finalizing:
Read more in CMS’s factsheet and the 2024 Physician Payment Schedule - From From DC: Medicare Dental Coverage Expanded, New Housing Supports Program, and More Justice in Aging, November 3, 2023. Additional material from the 2024 Physician Payment Schedule
New Video Explains Supplemental Benefits for Consumers Considering Medicare Advantage Plans Medicare Rights is pleased to share a YouTube video, made in collaboration with the National Council on Aging, addressing Medicare Advantage supplemental benefits. Watch it now to learn more about Medicare Advantage supplemental benefits, including what kinds of supplemental benefits exist outside of Original Medicare, when and how supplemental benefits may be available, and alternative ways to access similar benefits outside of Medicare Advantage plans. Watch or share the video: Understanding Medicare Advantage Supplemental Benefits - YouTube - From Medicare Rights Center.
Adult Shelters Overflowing Emergency homeless shelters that serve adults in Massachusetts are at or over capacity and on the brink of a crisis, according to shelter providers and advocates. Although the adult shelter population always swells as winter approaches, advocates and officials say in many places, the increase in individuals seeking shelter happened much earlier than normal and in larger numbers than expected. Facing what they says is a dire situation, several advocates and homeless service providers sent a letter to Healey calling for the state to open large overflow shelter facilities for the cold months. Anyone facing homelessness — from unaccompanied youth and adults to families — should have access to those emergency facilities, they said. "We are calling for a winter plan this year like never before, that will really provide some kind of emergency shelter response for all vulnerable people," said Joyce Tavon, CEO of the policy and advocacy organization Massachusetts Housing & Shelter Alliance. "Are there military bases, large sites that could be used for winter response?" The office of housing said 608 extra shelter beds for adults are coming on line across the state for the cold months — just over 200 of them beds that were not put up last winter. Extra beds are typically put up by some shelters, churches and municipalities across Massachusetts each winter, with some funding help from the state. But advocates fear the effort won't be enough this year. "I think I understand why [there's a] focus on families, because you cannot have kids out there in the cold," said Lyndia Downie, president and executive director of Pine Street Inn, a shelter and housing provider in Boston. "But at the same time, we don't want anybody to be out there in the cold, and we've all got to really figure out a way to get through the next few months." According to the Boston Public Health Commission, on Oct. 31 of this year, the number of people staying in adult homeless shelters in Boston was 16% higher than on the same date last year. Between 75 and 100 more men stayed at the Pine Street Inn's main shelter every night this October than on the same dates in 2022, according to the nonprofit's own data. The women's shelter has also seen an increase this fall. The state does not have an official count, but there are about 40 emergency shelters for unaccompanied adults in Massachusetts. They receive state funding, but are run by nonprofit organizations and in some cases public agencies, and they operate independently. That's different from the family shelter system, which is a network of facilities overseen by the state's Executive Office of Housing and Livable Communities. Many Factors Driving Increase in HomelessnessAdult shelter providers said some migrants arrived at their doors earlier this year, though the numbers remained manageable. Then, some said, they saw a notable increase starting in late summer to early fall. That may have been partly due to families starting to split up and send some members to adult shelters since the family shelters were full. Homeless service providers and state officials say high housing costs and the shortage of affordable housing in Massachusetts, along with the end of pandemic-era programs such as eviction moratoriums and stimulus checks, have contributed to the increase in homelessness. Efforts to clear the large tent encampment in the area of Boston known as "Mass. and Cass" have also contributed to the rising adult shelter population. Father Bill's & MainSpring, which operates adult and family emergency shelter and permanent supportive housing programs on the South Shore, said it's seen a 46% year-over-year increase in the number of adults who've stayed in one of their emergency shelters. The organization's shelters in Quincy and Brockton have seen populations in October and November that they normally wouldn't see until winter, according to president & CEO John Yazwinski. Just as alarming is the spike in the number of people staying on the streets, he said. "What we've seen is a 40% increase of unsheltered homeless people sleeping outside in our region, in Quincy, Weymouth, Brockton, Plymouth, Wareham," Yazwinski said. "That's the number we're worried about, whereas we're already in overflow [in our shelters], seeing people that we don't have enough beds — people are sleeping on the floor — what happens as we progress, where we don't want to turn anybody away?" Adults experiencing homelessness get bounced around like ping pong balls, she said, because there's no central clearinghouse for adult shelters in the state or way for people to apply for a bed, as families can do in the state shelter system. Unaccompanied adults have to call around or go from shelter to shelter looking for a bed. The two public shelters in Boston — the men's shelter at 112 Southampton Street and the Woods Mullen women's shelter — are open to all throughout the year, according to Jerry Thomas, director of the homeless services bureau of the Boston Public Health Commission, which runs the facilities. Some other shelters will bring in anyone who comes to their doors during the coldest days of the year. But not every shelter can accommodate all who come seeking help. "If someone shows up, we do not turn them away. If someone calls, we might tell them the situation and obviously urge them too see if there's another alternative," Thomas said. "That's what our primary mission is, to provide shelter ... so we want to do that. But we also don't want... [some] town's police dropping people off here or there, which does happen, because those towns aren't ... really taking care of their people." - See the full WBUR story.
Emergency Assistance Family Shelter Reaches New Capacity Limit; Families on Waitlist and Most Have Nowhere to Go As reported last month, Gov. Healey has placed a new capacity cap on Emergency Assistance (EA) family shelter. That capacity limit was reached early this month and there are now at least an estimated 90 families on the waitlist. The state has created one temporary overflow sites set up at the MassDOT building at 10 Park Plaza that can house 25 families, referred through EA, during the overnight only (and is currently slated to close on December 7). This week the Boston YMCA started providing those families daytime services from 8 until 2pm. The state also announced this month a partnership with United Way of Massachusetts Bay to administer a $5 million grant program for community-based organizations, faith-based groups, and volunteer organizations to stand up short-term, overnight shelter sites. Meanwhile, the $250 million that Healey requested in September to maintain emergency shelter operations has yet to emerge through a supplemental budget bill. House Democrats want to steer $50 million of that amount toward the launch of overflow shelter sites and force the Healey administration to revoke its shelter cap if it fails to launch such sites, while Senate Democrats didn't outline specific uses for the overall funds. The legislature has finished formal sessions for the rest of the year. While legislation can move forward in informal sessions, legislation can be blocked a by a single legislator. Formal sessions resume in early January. Waitlist Priority
Notification of available shelter Families on waitlist will be contacted by email, phone, and text using information family provided. They will be required to contact EOHLC by 12 pm the next business day to accept the offer or it will be offered to another family. (Families need to keep their phones charged!) - Sources and for More information:
Bill Would Allow Pay for Caregiving Spouses A bill before the Massachusetts Legislature seeks to expand the definition of family members eligible to be reimbursed through MassHealth programs. Currently, spouses are the only relationship excluded from that program. This legislation doesn’t affect program eligibility rules for enrollees, but broadens the definition of people who can serve as a paid caregiver. Note that the state legislature has ended formal sessions for the year. In informal sessions a single legislator can block bills. Formal sessions will begin again in early January 2024. Sen. Joanne M. Comerford, D-Northampton, introduced the bill to the Legislature’s Committee on Children, Families, and Persons with Disabilities, highlighting the need to allow spouses to serve as paid caregivers, especially given the extensive waiting lists for homecare services. "There are people on the waiting list, as you know, who can't get the home care they need,” Comerford said. “Allowing qualified spouses to serve as family members who provide the care will actually expand the pool of caregivers, which I imagine then would reduce the waitlist and allow more people to get the care they need to stay at home.” The bill would authorize the state’s Executive Office of Health and Human Services to seek a waiver from the federal government to make the change. Betsey Crimmins, executive director of Mass Home Care, finds several benefits from this provision. “If people are given a choice, many would choose to have their spouse provide care, if it didn't mean complete financial catastrophe for the family,” Crimmins said. “There's continuity of care, there's somebody that you know, somebody that you trust who's there and you don't have to worry about someone calling in sick or moving or quitting.” Home caregivers are less expensive than nursing homesCrimmins also mentioned that caregivers who qualify for Medicaid can see cost savings compared to nursing homes or institutional settings. “Nursing home care is both really expensive and it's where people end up having the worst health outcomes and average nursing home rates are $14,000 to $17,000 a month,” Crimmins said. “Within a couple of months, you've already paid out more for someone who's ... in an institutional setting where they don't want to be than what it would have cost to pay their spouse to stay home and provide the care to them for one whole year.” The shortage of home care workers across the country can also lead to dire consequences. The Executive Office of Elder Affairs wait lists show 4,396 people eligible for in-home services that were waiting for a provider, according to Crimmins’ written testimony. Another 718 found a provider, but were waiting for services, which can take several months. The federal government allows states to include spouses as paid caregivers in Medicaid programs. Fifteen states, including Vermont, California and North Dakota, have already embraced the change, showcasing the potential benefits of such legislation. - See the full Cape Cod Times article.
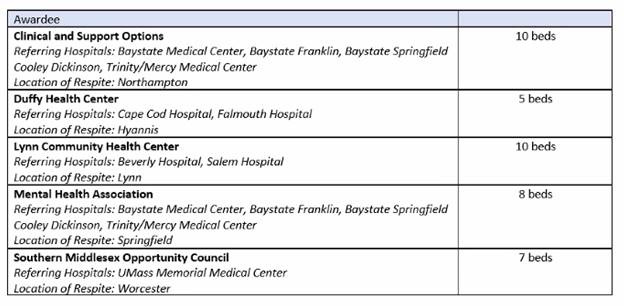
New Grants for Medical Respite Pilot Program, But Accept Referrals from Specific Providers/Geographic Areas Only The Healey-Driscoll Administration has awarded $5.2 million in grants to healthcare agencies and community-based organizations partnering to provide services to people experiencing homelessness. The grants are part of a new medical respite pilot program that provides individuals experiencing homelessness a safe space to recover after a hospital visit. Respite locations will offer 40 beds of temporary housing with clinical supports while program participants receive assistance in finding suitable long-term housing. “By working together with healthcare agencies and providers, we are not just improving the flow within our emergency departments and hospitals; we are offering residents a safe place to recuperate,” said Health and Human Services Secretary Kate Walsh. “The launch of this medical respite pilot program grant shows our commitment to providing quality healthcare and also addressing health-related social needs.” The services are similar to those offered by the Barbara McInnis house, but with the important difference that residents may stay for up to 6 months and receive assistance to seek permanent solutions to their lack of housing. The Medical Respite awardees include Clinical and Support Options, Inc.; Duffy Health Center, Inc.; Lynn Community Health Center and Lifebridge, Inc.; Mental Health Association, Inc. and Trinity Healthcare for the Homeless; and South Middlesex Opportunity Council and UMass Memorial Medical Center. None are in the Boston area. Each will accept referrals from their partner health care organization (see chart below). MassHealth’s Emily Cooper recently told a MHA case manager’s meeting that Boston area hospitals may refer patients from one of the geographic areas covered by the pilot, or who were transferred from one of those hospitals, and these patients will be considered if space is available.
Cooper also noted that no applications were submitted from Boston area hospitals during the procurement process and that “money was left on the table.” She encourages hospitals to think ahead for 2025, to partner with a homelessness provider and health center to and be prepared to apply if/when the program is able to expand and accept additional programs. - From The SUPPORT Act, Medical Respite Program, and more ..., MHA's WEEKLY WRAP-UP, November with additional material from MHA Case Manager’s meeting, 11/15/23.
MassHealth Programs to Help Wheelchair Users with Slow Repairs are Themselves Delayed Two pilot programs intended to address chronically delayed wheelchair repairs are themselves taking months longer than planned to launch. One pilot program would create a supply of loaner chairs that wheelchair owners could use while their primary chairs are being repaired. The other would establish a mobile team that could make simple repairs. Eventually, MassHealth would give more businesses, potentially including bike repair shops, access to Medicaid reimbursement for simple repairs. Painfully slow wheelchair repairs have become a nationwide problem. Several Massachusetts residents described waiting months for basic repairs, and living in pain or having their mobility severely curtailed in the meantime. Delays obtaining insurance authorization for repairs and scheduling complications play a role, but advocates say the $59.7 billion durable medical equipment industry has failed to properly invest in repair services, resulting in understaffed and overworked repair teams. State legislation introducing mandatory two-year warranties on new wheelchairs and requirements for companies to respond to repair requests quickly is under consideration in the Senate’s ways and means committee. “Expanding the options for people that are legal and covered by insurance such that they would still be eligible for a warranty and they don’t have to go outside the system to get timely repairs, that’d be ideal,” said Harry Weissman, director of advocacy at Boston’s Disability Policy Consortium. Bonnie Denis lives in Malden now, but while living in Somerville she occasionally relied on a local bike shop to change the tubes on her wheelchair tires. Wheelchair tubes are often interchangeable with those for bicycles, she said. The work cost $20, which she would pay out of pocket. Medicaid reimbursement for bike shops for small repairs would be a significant benefit, she said. “There are many people who can’t afford to do it,” she said. The two pilot programs are designed to run for three years, but they were going to be funded with $3.7 million in federal pandemic recovery funds that must be used by March 2025. Under the original timetable, that funding would have supported the first two years of operation. Because of the delays, though, that federal money will expire earlier in the life of the programs. MassHealth officials said they expect to find state revenue sources to support the program. Ironically, the company most likely to receive the contract to assist the pilot programs is one of those that now infuriate wheelchair users with their slow response to repair requests. The wheelchair industry is dominated by two large national suppliers, Numotion and National Seating and Mobility; those companies stand to benefit from the pilot programs’ success, Weissman said. Giving wheelchair users more places to get simple repairs should free larger providers to focus on more complex work, he said. Though wheelchair users already turn to bike shops, or handy friends, for easy fixes, many don’t realize that’s an option. MassHealth’s pilot program seeks to expand awareness of that resource, and assuage concerns that relying on a bike shop could invalidate the warranties on newer chairs. - See the full Boston Globe article.
Latino Children are More Likely to Enter Foster Care in Massachusetts Than Any Other State Growing up Latino in Massachusetts carries a greater risk of entering the foster system than anywhere else in the nation, and for those who end up in foster homes — as well as those who are the subject of child welfare investigations — the consequences can be devastating. For children, living in foster care is associated with an increased risk of entering the criminal justice system and worse educational outcomes, state and national studies show. Allegations of child mistreatment can also follow parents for years, hurting their ability to get jobs long after their DCF cases close. “Once the system gets a hold of us, it never lets go,” said Nelly Medina, herself a foster child and founder of Free Worcester, a nonprofit focused on educational justice and civil rights for disadvantaged children, including those in the Latino community. In Massachusetts, Latinos comprise just 20 percent of all children 17 and younger in the state, but 34 percent of children in foster care, according to data from the US Census and the Department of Children and Families. Their overrepresentation in the foster system is greater by far than any other state’s, according to an analysis of 2021 data by Child Trends, a national nonprofit researching issues affecting children. A more culturally sensitive child mistreatment reporting system and more resources for people in poverty would help stem the flow of Latino children into the child welfare system, say child advocates and activists from the Latino community. Also needed, they said, is more cultural awareness throughout the system. Cultural biases and language barriers cause Latino families to face added scrutiny, advocates for Latino communities and lawyers with Spanish-speaking clients said, and make navigating the child welfare system, with nothing less than the fate of children at stake, even more confusing. For parents, just being investigated by DCF can be traumatic, even when they’ve done nothing wrong. One out of every 20 Latino children in Massachusetts — almost 14,000 children — is the subject of an active DCF case, according to 2022 data, the most recent available. Latino children are slightly more likely than Black children, and more than twice as likely as white children, to have an open case with DCF. DCF officials insist workers aren’t biased, and point to data showing that after being referred to DCF, Latino families are no more likely to be cited for mistreating a child than any other demographic group. A root cause of Latino overrepresentation in the child welfare system, they said, is disproportionate reporting. State law requires professionals such as teachers, doctors, and child care providers to report suspected neglect and abuse, and they can face fines, and even jail, if they don’t. Referrals from these so-called mandated reporters account for about 80 percent of the child maltreatment allegations, or 51A reports, DCF receives. Once a 51A is filed, DCF is required to investigate, but too often DCF finds the conditions being reported are the result of poverty, not bad parenting, agency officials said. “Maybe you’re concerned about food, clean clothes,” said Mary McGeown, undersecretary for the Office of Health and Human Services. “There are lots of responses that can be put into place long before you contact the Department of Children and Families.” About 73 percent of DCF’s cases are neglect investigations, and lack of housing, child care, healthy food, or employment can all be interpreted as negligence, said Rachel Gwaltney, executive director of Children’s League of Massachusetts. No single demographic group in Massachusetts has a higher poverty rate than Latinos, according to the census. They also have the state’s lowest median household income. “We need to see more services for families that are culturally responsive,” Gwaltney said. “When you go and ask for help, any type of resources, all these places, are all mandated reporters,” said Tatiana Rodriguez, executive director of Family Matters First and a parent advocate with the Harvard Legal Aid Bureau. “They’re trained to overreport.” Rodriguez, a former foster child herself, calls it racism: “A Hispanic family cannot get away with what a white family can get away with, period.” Latino parents who aren’t fluent in English face challenges throughout the child welfare system. Families whose DCF cases don’t end up in court typically don’t receive court-appointed legal representation. If they can’t afford their own lawyer, they can face the child welfare system without a guide. Key documents aren’t always provided in Spanish quickly, and children are placed with foster families that aren’t from the same culture. Translated documents alone may not even help, if no one in the family can read or fully grasp the guidance. DCF requires cultural humility and sensitivity courses for all social workers, said Ryan FitzGerald, DCF’s chief of staff. “Issues of identity and diversity are central to children’s welfare, and it’s deeply grounded in our work,” he said. Just 16 percent of DCF’s administrators and professionals are Latino, though, according to the state’s employee diversity dashboard. - See the full Boston Globe article.
With Funding Challenges Looming, Mass. Child Care Could be in Jeopardy Pandemic-era federal funding for child care ended in September. Governor Maura Healey and the Legislature provided one-time state funding of $475 million to the industry through the end of the fiscal year in June. This year, the state separately also budgeted roughly $850 million — mostly from the federal government — to support child care financial assistance through items such as subsidies for low-income families and reimbursements to the providers who serve them. But providers said the child-care industry is so broken that it requires a more permanent funnel of government money that goes directly to providers, such as the Commonwealth Cares for Children grants that came through during COVID-19. The American Rescue Plan and other COVID funds funneled more than $600 million directly to child-care centers using a formula that accounted for staffing levels and community demographics. It helped keep businesses afloat amid fiscal freefall. Now, providers said, the coming end of the C3 grants means centers from Granby to Chelsea will likely have to hike tuition to cover overhead expenses, including rent, insurance, and supplies. Teachers — already paid no more than $46,000 annually — will likely have to soldier on without wage increases or leave the industry out of necessity. Some centers fear they will have to accept fewer children from low-income families, whose government subsidies do not cover the full cost of care. Others warn they may be forced to close. Bills winding through the State House aim to combat the problems by creating new state funding, expanding subsidies for families, and debuting publicly funded early childhood education. A spokesperson for the Healey administration said the governor supports legislative efforts to make early education more affordable and accessible, and would review any bills that reach her desk. Without them, the additional money from C3 grants acts as little more than a Band-Aid, said Stephen Huntley, president of the Massachusetts Association of Early Education and Care. “The federal money bailed us out at a time when we needed it, but the need has just gotten worse,” Huntley said. “The pendulum could swing 180 degrees in the wrong direction quickly.” Throngs of providers see the C3 grants not as a benefit but rather an “indispensable tool” to keep centers open, said Amy O’Leary, executive director of the advocacy group Strategies for Children. Providers across Massachusetts say the grants helped them stave off tuition increases and accommodate children with greater needs. Should legislators find a replacement for the money, 81 percent of Massachusetts center-based providers would increase salaries for educators, according to a survey from the nonprofit Neighborhood Villages. One in eight providers would consider reducing tuition. The end of C3 grants, providers worry, could exacerbate the cost of care even further and drive working parents into full-time caregiving. “It’s going to disproportionately impact those single-income homes, which again will impact women of color,” said Sandra Quince, chief executive of Paradigm for Parity, a coalition of business leaders addressing the gender gap in the C-suite. Expanding funding for child care would lead to increases in the number of employed parents and the hours they work, a study from the University of Massachusetts Boston found. The percentage of infant and toddler mothers employed in the state would rise from 70.5 percent to 74 percent, the study said. - See the full Boston Globe article.
Patients Don’t Know How to Navigate the US Health System - and it’s Costing Them Of all the culprits that make it harder for Americans to afford and access health care, the sheer confusion many patients experience when trying to select an insurance plan or when faced with an expensive medical bill may be the most overlooked. That’s according to a recent survey from research firm Perry Undem, which reveals the deep confusion Americans feel when receiving health care — confusion that could put them on the hook for higher costs. The Perry Undem survey, which polled nearly 2,700 Americans on behalf of the American Cancer Society’s Cancer Action Network, the Leukemia and Lymphoma Society, and RIP Medical Debt, also detected widespread struggles to afford health care. About 7 in 10 people say they have received a medical bill that they could not afford, it found, and more than 60 percent of Americans said they had made some kind of sacrifice — delaying care, skipping appointments, changing the food they buy at the grocery store, etc. — in order to afford health care in the past two years. New data, from Perry Undem and from the health policy think tank KFF, further indicates that Americans have a lot of misconceptions about how their health care and insurance benefits are supposed to work, and could find themselves exposed to higher costs as a result. More than half of Americans said they were either always, frequently, or sometimes uncertain about whether they had been seen by an in-network provider when receiving medical care. If they were treated by an out-of-network doctor, most insurance plans will charge the patient more money out-of-pocket for those services. Those front-end issues — seeing a doctor or receiving a service not covered by your insurance plan — can create big medical bills in the first place. But patients also often don’t know what to do when they receive an invoice they can’t afford. Only 3 in 10 Americans said they had fought or appealed a medical bill they had received. The survey reveals wide disparities in who has actively worked to reduce their health care bills: Older Americans, people with a college education, and white Americans were roughly twice as likely to say they had contested a medical bill than young adults, people without a college education, or Black Americans. Why are so few Americans fighting back against exorbitant medical costs, even though 70 percent of those who did said they were successful in reducing their balance and experts like investigative journalist Marshall Allen have pleaded with patients to “never pay the first bill”? Once again, confusion is to blame: 23 percent of respondents said they didn’t know they could fight a bill, 19 percent said they didn’t know the steps to take, 17 percent said that the process was overwhelming, and another 12 percent said they were too busy to contest a bill. Many Americans are also ignorant of the financial assistance that may be available to them: Nearly half of the people surveyed were not aware of the programs run by hospitals or physician practices that are meant to help patients pay their share of their bills. Only one in four said they had actually asked for or been offered such assistance. KFF’s Larry Levitt and Drew Altman recently wrote in JAMA Forum that complexity in US health care is “the enemy of access and affordability,” citing results from a KFF survey taken over the summer. About 6 in 10 Americans said they had experienced a problem using their health insurance in the past year, according to KFF. People reported being unable to receive care, experiencing a decline in their health, and/or paying more than they expected for treatment as a result of those insurance problems. In findings similar to those of Perry Undem, the KFF survey found 60 percent of Americans didn’t know they can appeal a medical bill. The confusion starts during open enrollment, as Levitt and Altman noted, when people enrolling in Medicare Advantage have more than 40 plans available to them, on average, and people who sign up for coverage on the Affordable Care Act’s marketplaces may have more than 100 to choose from. HR industry surveys have also found that people who enroll in health insurance through their job often feel uncertain about the selections they are making. And it continues as people actually receive medical treatment and then receive a bill, as evidenced by these findings. People don’t know if their providers are in-network or that they can contest a bill, and they may end up paying more than they should as a result. These surveys suggest that Americans remain perplexed by the process of seeking out medical services and paying for treatment — and their health is suffering as a result. - See the full Vox article.
Healey Proposes Mass Rehab Name Change to MassAbility to Reduce Stigma Gov. Maura Healey has proposed renaming a 67-year-old state agency, a switch that she says will remove stigma surrounding individuals in the disability community and boost their employment opportunities. The Massachusetts Rehabilitation Commission would be renamed MassAbility, under a new bill filed this month. "Rehabilitation is a term that is no longer relevant to the work" of the agency, she said, and connotes that "something is wrong or needs to be fixed." "It will modernize the language across all enabling statutes with the aim of removing outdated and stigmatizing terms. These changes will provide clarity and consistency." Healey said at a press conference. The name change requires legislative approval. The commission provides job preparation for students ages 14 and older, in addition to the Vocational Rehabilitation Program to support individuals in the workplace who have physical, cognitive, intellectual or mental health conditions. The agency also helps people navigate their disability benefits, offers assistive technology like wheelchairs and car modifications, and provides services to allow people with disabilities to live in their communities. The MassAbility renaming proposal reflects research, including focus groups, surveys and conversations, with the disability community, businesses, providers and advocacy groups, according to Healey's office. The governor's legislation would also remove from statute the words "handicap," "handicapped" and "retarded," according to Healey's filing letter. Those would be replaced with "barrier," "person with a disability" and "person with intellectual disabilities." Healey also proposed to repeal what her filing letter described as the commission's "antiquated, and now non-existent, program for extended sheltered employment for people with disabilities." "The name 'MassAbility' captures all the untapped potential that's unlocked by the agency's employment and independent living services," said Health and Human Services Secretary Kate Walsh. "MassAbility conveys the message that employees with disabilities have unique lived experience, perspectives, skill sets, mindsets and representation." - See the full WBUR story.
Apartment Application Fees Add Up- and Some are Illegal Amid a region-wide housing shortage, advocates say application fees are on the rise, even when they're not allowed. Massachusetts is one of the only states where it’s illegal for landlords to charge application fees. But with little enforcement of the law, advocates say these charges are becoming an entry fee to finding an apartment. Housing activist and real estate agent Carlos Betancourt spends much of his time helping low-income renters find apartments. He said the majority of places he sees charge application fees. Betancourt explained how it often works: A listed apartment will come with an application fee of $25 to $70 — per adult. And, he said, that's frequently just to view the place. He remembers attending an open house where everybody interested in the apartment had to pay. The open house lasted three days. Friday, Saturday and Sunday, "they were taking applications," Betancourt said. "One month later, they did another open house. So how many people went over there?” If brokers accept fees from multiple applicants and don't refund them to people who aren't vetted for the apartment, "it's unethical but it's legal," according to Andrea Park of the Massachusetts Law Reform Institute. The MassLandlords website explains the restriction this way: "Largely because the Realtors have a better lobby than we do, brokers can charge application fees." Adding to the confusion, scammers are taking advantage of apartment hunters, posing as landlords in online ads that call for fees with applications. Some states set limits on application fees, but Attorney Ariel Nelson of the National Consumer Law Center in Boston said Massachusetts and Vermont appear to be the only ones that bar landlords from charging them outright. Here, the only fees landlords can legally charge are first and last month’s rent, a security deposit and the cost of changing locks. Advocates complain it’s often up to tenants to see that the prohibition on application fees is enforced. Ariel Nelson said that’s a tall order for low-income renters struggling to find an apartment. She wants to see attorneys general doing more enforcement. Doug Quattrochi, head of the advocacy group MassLandlords, acknowledges that application fees have cropped up more. A highly competitive rental market is driving some of that, he said. In addition, some landlords feel justified charging for background checks, because it's increasingly difficult to evict bad tenants, and owners have to thoroughly vet applicants before handing over keys. Tenant advocates say renters can complain to the attorney general's office. They can also try to negotiate on the fees, or sue the landlord. But for renters desperate to find an apartment, those may not seem like great options. "What good does it do to complain to a landlord that the application fee is unlawful," Quattrochi said, "when you're trying to sweet talk them into letting you sign a rental agreement?" - See the full WBUR story.
|