|
MGH Community News |
|
MGH Community News |
| February 2024 | Volume 28 • Issue 2 |
Highlights
Sections Social Service staff may direct resource questions to the Community Resource Center, Hannah Perry, 617-726-8182. Questions, comments about the newsletter? Contact Ellen Forman, 617-726-5807. |
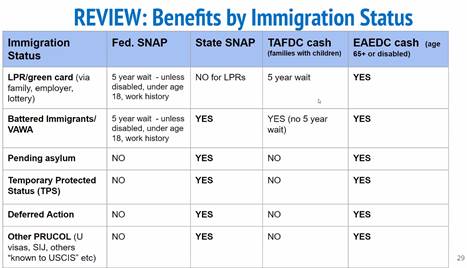
State SNAP for Certain LEGAL Immigrants Now Available
As reported last month, the federal government restricted legal immigrant access to SNAP benefits in 1996 and for a time (1997 – 2002) MA paid to maintain those benefits using state funds. Those benefits were subsequently cut, but are now being partially and temporarily reinstated via inclusion of $6M in the state Supplemental Budget signed in December. DTA is now issuing benefits to those eligible who have applied. The first round of payments were issued on February 15. Here are some application scenarios and how they are being handled:
Notices May Be Confusing Who’s Eligible The following groups are NOT eligible for FEDERAL SNAP: ADULTS with TPS or Humanitarian Parole from most countries other than Cuba/Haiti, those with pending asylum applications (again if not from Cuba/Haiti) and others who fall under the benefits informal grouping of “Permanently Residing Under Color of Law” (PRUCOL). Most (but not all) of the recent arrivals from Haiti qualify for federal benefits under special rules for “Cuban/Haitian immigrants”. Immigrants eligible for the state-funded benefit are legally present immigrants who cannot get federal SNAP including those with Humanitarian Parole or battered immigrants, as well as immigrants in the “PRUCOL” category. |
Federally “Qualified” immigrants who are subject to a 5 year bar including adult parolees and battered/VAWA immigrant adults would be eligible for state SNAP if otherwise eligible. Unfortunately, other ADULT Legal Permanent Residents (LPRs/green-card holders) who are subject to the 5-year waiting period will still NOT be covered under the state-funded benefit. PRUCOL examples for state SNAP eligibility:
This is not a complete list. Note that this definition of “PRUCOL” varies between programs and may not be the same definition for other benefits such as MassHealth and Emergency Assistance (EA) family shelter.
This is a Temporary Benefit State-funded SNAP is available for the fiscal year (ending June 30, 2024) or when the allocated funds are exhausted- whichever comes first. More Information and Sources
- From [FoodSNAPcoalition] UPDATE: State SNAP for Immigrant Households and MLRI/GBLS training tomorrow!, Pat Baker, MLRI, February 14, 2024 and [FoodSNAPcoalition] SNAP Coalition meeting 2/27 & Important SNAP Updates and Trainings!, Pat Baker, February 21, 2024.
Moving and Advancing of Massachusetts and Connecticut Immigration Court Hearings – Immigrants Should Check Their Court Date and Location On April 8, 2024 the Executive Office for Immigration Review (EOIR) will be opening a new immigration court in Chelmsford, Massachusetts (the “Lowell Immigration Court”). In the coming weeks and months, EOIR will be pulling cases of individuals who reside in certain zip codes from the Boston and Hartford Immigration Court dockets and transferring them to Lowell. Because the Lowell court will have a complete slate of new cases, cases on the Lowell docket will likely proceed much more quickly than cases have in Boston and Hartford. When cases are transferred, the Boston/Hartford hearing dates will be canceled, and it is very likely that the rescheduled date will be significantly sooner. And because cases will be removed from the Boston and Hartford dockets, it is likely that cases which remain in those courts will also be advanced when hearing slots from transferred cases open up. Expedited dates can be good news or bad news for immigrants, depending on the outcome of the hearing. If you have a case pending in the Boston or Hartford courts, we strongly recommend that you check the EOIR online portal regularly to check your client’s next hearing date. - Adapted from URGENT: New Lowell Immigration Court Opens in April - Pro Bono News (February 2024), Melanie at PAIR, February 1, 2024. Thanks to Fiona Danaher for forwarding.
New Biden Loan Forgiveness to Save Mass. Borrowers $19.5M Nearly 2,500 Massachusetts borrowers will see millions of dollars in college debt wiped out under President Joe Biden’s new $1.2 billion loan forgiveness cancellation program. Under the program, borrowers with less than $12,000 in student loans and who have been making payments for at least 10 years would get their remaining loan balance erased if they enroll in the federal government’s Saving on a Valuable Education repayment plan. In Massachusetts, the plan will cancel $19.5 million in college loan debt held by 2,490 borrowers, according to data provided by the Biden administration. For every $1,000 borrowed above $12,000, a borrower can receive forgiveness after an additional year of payments, according to the Biden administration. All borrowers who have signed up for the SAVE program will receive forgiveness after 20 or 25 years, depending on whether they have loans for graduate school. The Biden administration said the forgiveness is based on the principal balance of federal loans borrowed as a student to attend school, “not what a borrower currently owes or the amount of an individual loan.” Overall, Biden’s latest loan forgiveness program will cancel up to $1.2 billion nationwide. To date, $136.6 billion in federal college loans have been forgiven for more than 3.7 million Americans, according to the Biden administration. In June, the U.S. Supreme Court struck down a Biden plan that had called for canceling up to $10,000 in debt for those earning less than $125,000 per year and up to $20,000 for those who received federal Pell Grants. In a 6-3 decision, the high court ruled that the administration overstepped its authority in attempting to cancel or reduce student loan debt, effectively ending the $430 billion plan that would have canceled up to $20,000 in federal student loans for 43 million people. Conservative groups have filed legal challenges to Biden’s other loan forgiveness plans, but so far they haven’t been successful. Recent studies suggest that decades of declining financial aid support is putting many college students in deep debt. Massachusetts has cut state financial aid by 47% since 2002, according to the report, as other states have increased it by an average of 15% per student. The National Association of State Student Grant and Aid Programs ranked Massachusetts 37th in the nation in terms of providing funding for student financial aid, trailing far behind top-spending states such as Kentucky, Georgia and Louisiana. - See the full Newburyport News article.
Major Barriers Persist for Formerly Incarcerated People Who Need IDs Supreme Hassan says he was released from prison in August without a state-issued ID — a document considered crucial to succeeding outside of prison walls. The 51-year-old, whose birth name is Jeffrey Hilton, left prison after 33 years excited to start his new life. He moved to a halfway house in Boston. But several months later, he says he still struggles to create the building blocks of his new life, like opening a bank account or applying for jobs. “Without a state ID, I just do not exist within the commonwealth of Massachusetts,” Hassan told GBH News recently. It’s not supposed to be this way. Last March, Massachusetts officials announced an initiative known as the Enhanced State ID Program to make it easier for people returning from state prison to obtain official identification. But almost a year later, former prisoners and their advocates say the agreement has not fixed the system and too many people are still leaving prison without the proper documents they need to get along on the outside. The Department of Correction told GBH News that it helped 572 former prisoners get state IDs in 2023, a fraction of an estimated 3,500 people released from state prison last year. Prison officials point out that number doesn’t include people being released who already had documents or were not eligible for IDs for other reasons. And the rate of prisoners receiving IDs has increased substantially over the last five years. In 2019, 262 people got IDs with the state’s help, state officials say, less than 4% of more than 7,000 prisoners released. But the process still is marred by roadblocks, many advocates say, including requirements that eligible applicants have a record on file with the state Registry of Motor Vehicles and a Massachusetts residential address where they are scheduled to live upon release. State prison officials say they are working with the RMV to finalize plans for a mobile unit that would go to prisons so that individuals can create RMV accounts and immediately become eligible for the program. State Rep. Brandy Fluker Oakley, a Democrat from Boston, told GBH News that more needs to be done. She says these conditions still create barriers for prisoners who came to Massachusetts from out of state and those without a local address to return to. To improve the process, Fluker Oakley is sponsoring a bill that would ensure that government officials begin the application at least 120 days before a person is released from state prison or county jails. This would give reentry staff time to gather documentation, like a birth certificate or social security card, at the prison or jail. The bill also would expand the list of addresses an applicant could use to apply for an ID, including temporary shelters, places of worship, or homes of family and friends. And the legislation stipulates that the RMV must accept an ID issued by a prison or jail as acceptable proof of Massachusetts residency. - See the full WGBH story.
Mass. Doctors Hail New Federal Rule Expanding Access to Methadone The Biden administration earlier this month approved a new federal rule that allows many patients to take methadone home with them, freeing them from having to visit a clinic each day. Starting April 2, when the rule takes effect, people will for the first time be allowed to start on methadone after an audio-visual telehealth consultation, rather than an in-person visit, and would be able to receive much larger doses of the drug than previously allowed — alleviating painful withdrawal symptoms and, officials hope, helping to prevent potentially deadly relapses. The rule also loosens access to buprenorphine, another proven opioid treatment medication, by allowing telehealth providers to prescribe the medication without a medical visit. The long-awaited changes — some of which were adopted as emergency measures during the pandemic and now will be made permanent — are the most significant expansion of methadone access in more than a generation, and could help turn the tide on opioid abuse and fatal overdoses, say addiction treatment specialists, state officials, and clinicians across Massachusetts. “It’s a game changer,” said Dr. Ruth Potee, medical director for substance use disorders at Springfield-based Behavioral Health Network Inc., which runs four methadone clinics in Western Massachusetts. “Methadone, which is the gold standard for treating opioid use disorder, is finally being taken out of the shadows.” Methadone is one of three medications approved to treat opioid use disorder, and for many patients it is the only effective option. The drug is a synthetic opioid that lessens the often excruciating, nausea-inducing symptoms of withdrawal while blocking the high that users get from using opioids such as heroin and fentanyl. An expansive 2018 study analyzing data from 17,568 adults in Massachusetts who survived an overdose found that opioid overdose deaths dropped by 59 percent for those receiving methadone. Yet despite a dramatic overall rise in fatal overdoses in the past two decades, only about one in five American adults with opioid use disorder receive methadone or other medications to treat it, researchers have found. Access to methadone has been impeded by Byzantine rules dating back to the Nixon administration, which viewed the drug as a tool to control crime rather than a way to treat addiction. At the time, the rules were largely written by government officials and not doctors on the front lines of treating addiction. Starting in 1972, patients had to report to specialized clinics known as opioid treatment programs to get doses of the medication, typically dispensed under tight surveillance. Those restrictions have long stigmatized methadone and have forced people who use it to congregate in marginalized areas, such as the intersection of Massachusetts Avenue and Melnea Cass Boulevard in Boston, which has multiple methadone clinics. There are 55 opioid treatment programs in Massachusetts, mostly located in urban areas. Eighty percent of US counties don’t have any clinics that dispense methadone, according to a 2019 analysis by the Congressional Research Service. “These [methadone] regulations were never built on a scientific foundation,” said Leo Beletsky, a professor of law and health sciences at Northeastern University. “And in the middle of a historic overdose crisis, we have continued to make people bend over backwards and comply with rules that few people can reasonably meet.” Deirdre Calvert, director of the state Department of Public Health’s Bureau of Substance Addiction Services, experienced the onerous regulations firsthand when she ran a methadone program near downtown Boston in the late 1990s. Then, as now, patients had to demonstrate that they were misusing opioids for at least a year before they could receive methadone. Some patients would bring letters from their parish priests to document their addictions — a requirement eliminated under the new rule, she said. Though Calvert lauded the new rule, she said it still doesn’t go far enough. People will still be dependent on a small number of heavily regulated opioid treatment centers to receive methadone, even though the new rule allows them to take supplies home at larger doses. Like many addiction specialists, she supports proposals that would allow doctors to prescribe methadone and pharmacists to dispense it, just as they do for medications that treat other ailments. Clinicians have also long complained that federal limits on methadone doses are too low to be effective against powerful opioids like fentanyl. Current regulations recommend that clinicians start patients on 30 milligrams of methadone, a level that leaves people who use fentanyl with significant withdrawal symptoms, say clinicians. The new rule allows patients to start at 50 milligrams and doctors can use their discretion to go higher. The new regulation also eliminates the longstanding stricture that people must experience opioid addiction for at least a year before receiving methadone. That rule had stark consequences in the fentanyl era, in which even small delays in treatment can prove deadly, say clinicians. - See the full Boston Globe article.
Commercial Health Insurance Special Enrollment Period Extended Due to MassHealth Redeterminations The MA Division of Insurance has issued Bulletin 2024-04, which extends the special enrollment period for anyone who lost MassHealth coverage during the redetermination process, and who has subsequently been determined eligible for a commercial health plan (e.g., Blue Cross and Blue Shield and Health Maintenance Organizations). Those individuals have until November 23, 2024, to enroll and the bulletin instructs insurers to “take all necessary steps” to facilitate the enrollment. Excerpts from the Guidance: Those persons who would be redetermined as ineligible for MassHealth coverage were identified as a population who may be vulnerable during the transition off MassHealth coverage. The process of redetermining MassHealth members has continued into calendar year 2024, and concerns about individuals transitioning out of MassHealth and into other coverage also have continued into 2024. Therefore, in the interest of facilitating a smooth transition back to commercial health insurance, the Division and the Health Connector have designated a temporary triggering event for (1) any individuals who lose MassHealth during calendar year 2024; and (2) any individuals who lost MassHealth on or after April 1, 2023 and who have since been determined eligible for an MGL c176j health plan (small group health plans), but who remain unenrolled in a health plan. The special enrollment period for these individuals is extended to November 23, 2024, for coverage becoming effective in 2024. See Bulletin 2024-04. - Adapted in part from MHA's WEEKLY WRAP-UP, February 2, 2024.
People Can Get Even More Medicare D Extra Help in 2024 Beginning this year, the Inflation Reduction Act (IRA) expands eligibility for the Part D Low Income Subsidy (LIS), also called “Extra Help.” This important program helps people afford their medication and coverage. New in 2024, everyone with Extra Help will pay a $0 premium, $0 deductible, and a reduced amount for both generic and brand-name drugs. To qualify for Extra Help, people must, in most cases, live in one of the 50 states or the District of Columbia, and have income and resources below a certain limit. For 2024, an enrollee’s monthly income must be below $1,903 for an individual ($2,575 for a couple). Resources—which include stocks, bonds, and money in a checking, savings, or retirement account—must be below $17,220 ($34,360 for a couple). Some people—those enrolled in Medicaid, Supplemental Security Income (SSI), or a Medicare Savings Program (MSP)—automatically qualify for and are enrolled in Extra Help; they do not have to apply. Others can apply at any time, either online ssa.gov/extrahelp or by calling Social Security (1-800-772-1213). For more information about Extra Help and other ways to lower drug costs, visit the Department of Health and Human Services’ newly launched resource hub at LowerDrugCosts.gov. Visit Medicare.gov/extrahelp or call 1-800-MEDICARE (1-800-633-4227) to learn about Medicare drug plans, Extra Help, and other ways to lower your prescription drug costs. TTY users can call 1-877-486-2048. Learn more about Extra Help and how to apply from Medicare Interactive.
Medicare Reminder: Phases of Medicare Part D coverage There are four different phases—or periods—of Medicare Part D prescription drug coverage:
Note: If you have Extra Help, you do not have a coverage gap. You will pay different drug costs during the year. Your drug costs may also be different if you are enrolled in an SPAP. - From Medicare Watch: Action Still Needed to Protect Critical Medicare Outreach!, Medicare Rights Center, February 15, 2024.
Shelter in Roxbury Rec Center Fills Up Quickly A newly opened migrant overflow shelter at a Roxbury community center quickly reached its 400 person capacity this month. Over their first weekend at the Cass, roughly 75 young people were enrolled in Boston Public Schools the mayor said. A different community center has taken on some of the Cass's programming, Wu said. Some tennis programs were relocated to spots in Jamaica Plain, she said. A youth track club at the Cass now has a schedule to meet in various locations, an arrangement that Wu described as "really not ideal." "I keep saying this is not a problem about migrant families. This is a problem about housing that we had before anyone came, that we have across every community," the mayor said. She added, "We are a place where that housing barrier for our own residents is tens of thousands of people on the waitlist for BHA," referring to the Boston Housing Authority. By mid-month the waitlist for Emergency Assistance family shelter was reported to include almost 750 families. - See the full WBUR story.
La Colaborativa Day Shelter Serving Migrant Families Opens in Chelsea – Exceeds 200-Person Capacity in First Day Within the first day open, a new La Colaborativa day shelter in Chelsea serving migrant families and homeless individuals exceeded its 200-person capacity by around 70 people and opening a contingency overflow site, staff told the Herald. “There is an inexpressibly heartbreaking level of need,” said Alex Train, chief operating officer at La Colaborativa. “That’s prevalent amongst all the households we met with today. Many have arrived very recently with only a couple of bags of essential items, without employment prospects nor stable housing. They’ve been forced to sleep on the sidewalk, sleep in Logan Airport or sleep in overflow shelters.” La Colaborativa announced it would open a day shelter with funding through the United Way of Massachusetts Bay and Healey administration earlier in the month. The funding comes out of a $5 million grant program through a state and United Way partnership announced in November after the state reached its 7,500 shelter cap. The program provides funding community-based, faith-based and volunteer organizations for short-term and overnight shelters. The shelter, which only operates daytime services, coordinates with the state to transport migrant families from the overflow state-run overnight shelter in Cambridge. In the first day, the shelter received about 211 families primarily from the Cambridge site, Train said, as well as 50 to 60 people from the area come in. La Colaborativa staff activated a contingency overflow site at their headquarters Tuesday to accommodate the influx, Train said. The shelter provides everything from hot meal services to assistance with mental health care, housing programs, work authorizations and more, Train said. The goal, he said, is a “intensive workforce development-oriented program” offering ESL classes, resume assistance, job interview training and the like, in addition to the wraparound services. When families came in Tuesday, they went through comprehensive intake and triage services to assess immediate needs and stabilize emergencies. During the process, Train said, several people were sent for emergency medical care. For about half an hour Tuesday, a father sat with his three-year-old daughter looking uncomfortable, Train said. The team that spoke to him found that he was unable to walk, hadn’t had a meal in many days and had had no access to health care before calling an ambulance. - See the full Boston Herald article.
Opinion: Gov’s Proposed PCA Cuts May Deny Services to Thousands of People with Disabilities Last month saw the release of the governor's proposed budget, and it was very much a mixed bag for people with disabilities. On the plus side, the budget includes additional funding for wheelchair repair, as well as increased funding for agencies that provide various social care services, which will hopefully spur increased hiring and help resolve staffing shortages. Unfortunately, the proposal also calls for cuts to the PCA program that would reduce spending by approximately $100 million compared to maintaining currently policies. MassHealth's plan to achieve these cuts is to slash weekly meal prep hours for everyone in the program from 13 hours to 7 hours, and to deny eligibility to any adult who has fewer than 10 hours per week of assessed Activities of Daily Living (ADL) need (i.e. activities such as bathing, dressing, feeding, and transfers), shunting these applicants into the Adult Foster Care and Home Health programs instead. (Services for children cannot legally be cut because of federal regulations.) We earnestly believe that MassHealth officials tried their best find the least damaging way to make these cuts, which we appreciate. Unfortunately, there is simply no way to take this much money out of the program, and these proposed measures will cause real harm to people with disabilities. Firstly, one hour a day of meal prep assistance is not remotely sufficient for many members who have complex dietary needs or need to have their food cut into small pieces or blended in order to be able to safely consume it (it may also negatively impact members with children.) Secondly, the 10-hour eligibility threshold will result in thousandsof people no longer being eligible for the PCA program. The harm will fall particularly hard on adults who are autistic, have developmental disabilities, learning disabilities, or traumatic brain injuries. This is because members of these communities often need lower levels of help with ADL needs but higher levels of Instrumental Activities of Daily Living (IADL) need, such as taking medication, organization, cleaning, and paying bills—and IADL need is not taken into account for the cutoff. As such, many members of these communities will find themselves booted from the program, as will people with many other types of disabilities. We are not convinced that the people who are denied PCA care will get their needs met by the other programs that MassHealth is saying will serve them instead. The Adult Foster Care program, for instance, requires that someone have a live-in family member or friend (who cannot be a guardian or spouse) who is willing and able to provide care, which would not be the case for many of the people losing eligibility. Meanwhile, many home health agencies already have waiting lists, and the advocates and experts we spoke to were deeply skeptical that that program would be able to effectively absorb thousands of people who were previously receiving PCA services. Even if they could, however, home care programs (while valuable) are by no means an ideal substitute for PCA care: they provide fewer services and dramatically less consumer control, meaning that many people with disabilities would be significantly less able to have a say in how they receive care. For all these reasons, we believe these cuts are harmful and inappropriate, especially just one year after this state spent a billion dollars on tax cuts. The budget should not be balanced on our community's back. - From BCBS Report calls for Estate Recovery Reform, Disability Policy Consortium Update, ckillick@dpcma.org, February 9, 2024.
Mass. Burdens Poor by Overly Aggressive Policy to Recoup Medicaid Costs After Death Nearly two years after her father’s death in 2016, Sandy LoGrande received a letter from MassHealth that left her stunned. It demanded $177,000 from the estate of her father, Salvatore “Sam” LoGrande, for Medicaid expenses he incurred during his battle with prostate cancer. LoGrande and her younger sister, Laurie LoGrande, didn’t have that kind of money. Their only option, she said, would be to sell the single-family Colonial in Gloucester their father bought in 1976. It was part of their inheritance, and LoGrande has continued living there since her father’s death. “I can’t believe that an organization that’s supposed to help people get a leg up is doing this,” LoGrande remembered thinking. Under federal law, state Medicaid programs are required to seek reimbursements for some Medicaid expenses from the estates of the deceased, but MassHealth has one of the more aggressive approaches in the country. There’s no limit on how much Massachusetts can try to recoup, and for some the bill can total hundreds of thousands of dollars — effectively draining the estates of many families. Now, the Blue Cross Blue Shield of Massachusetts Foundation and a consultancy that specializes in health care policy, the Aurrera Health Group, are calling out Massachusetts for its aggressive practices, arguing in a recent report that they unduly burden poorer families and rob them of the opportunity to build intergenerational wealth. “The emotional and financial consequences for the low-income families involved can be really devastating,” said Katherine Howitt, director of the Massachusetts Medicaid Policy Institute, an independent policy organization that is part of the Blue Cross Blue Shield of Massachusetts Foundation. Federal law does require states to seek recovery of Medicaid expenses, specifically for long-term care or services provided to people 55 or older, including those who lived at home, as well as people of any age who permanently lived in a long-term care or medical facility. Massachusetts goes even further: for that same population it seeks to recover, with some exceptions, every Medicaid expense incurred, not just those related to long-term care. That can include preventative procedures and care for chronic conditions. It is one of 23 states with estate-recovery policies that exceed federal requirements, according to the foundation report. Policy analysts and a state legislator say that even changes introduced in 2021 to exempt estates below certain amounts and expand eligibility for waivers did not go far enough to help low-income families. The report from the foundation and Aurrera looked to other states’ approaches to estate recovery. Its recommendations included waivers for property that is survivors’ sole income-producing asset, making it easier for a person’s caregiver to obtain exemptions, and exempting $25,000 from every estate eligible for recovery. In its statement, MassHealth said it would consider the report’s recommendations. “MassHealth, in its administration of the estate recovery program, seeks to prevent undue hardship for members and their families, promote intergenerational transfers of wealth for financially vulnerable heirs, and increase awareness about estate recovery requirements,” the statement said. The 2021 reforms exempted estates worth $25,000 or less and introduced additional waivers, and combined, are expected to halve the amount the state collects through estate recovery, from more than $47 million in 2019 to an anticipated $23.5 million. Before those changes, Massachusetts gathered more from members’ estates than any other state. Another important change, Howitt said, was an added emphasis on ensuring Medicaid recipients were aware of the possibility of estate recovery. The revenue lost to any additional changes would have minimal impact on MassHealth’s services, Howitt said. The state keeps only about half of what it recovers, with the rest reimbursing the federal government. The loss of revenue from the 2021 changes hasn’t directly affected MassHealth, the state said, since the money collected through estate recovery instead goes into the general fund, which finances a wide assortment of services. LoGrande and her younger sister fought MassHealth in court, and two years later reached a settlement that exempted them from paying the Medicaid expenses. They kept their father’s home. - See the full Boston Globe article.
Opinion - Bear Mountain Nursing Home Report Alleges Neglect, Overmedication; State Must Do More A nursing home can be a supportive environment for elderly residents to live out their last years with companionship and medical care. It can alternatively be a place where vulnerable people with severe physical and mental health needs are warehoused and neglected. A report released this month by the Disability Law Center examining a neurobehavioral unit at Bear Mountain nursing home in Worcester illuminates in stark terms what allegedly happens when people with schizophrenia, dementia, and other ailments are left alone, with few programs and inadequate staffing. The Disability Law Center writes, speaking broadly about nursing home patients, “They become vulnerable to abuse and neglect because of inadequate staffing and clinical expertise, excessive use of medication, substandard conditions, and prolonged isolation.” The report, while difficult to read, cries out for a response — from Bear Mountain and the state. Lawmakers and state administrators have responded to nursing homes’ financial needs by increasing reimbursement rates. But as the report points out, rates need to be paired with oversight to ensure the money is going to provide at least a minimal standard of care. Advocates with the Disability Law Center, which has legal authority to monitor Massachusetts organizations serving people with disabilities, said they began scrutinizing Bear Mountain because of complaints about staffing. But the issues identified are emblematic of larger problems. “You have a for-profit long-term health care system taking people who are complicated and for whom nursing homes aren’t primarily prepared to be caring for,” said Nina Loewenstein, senior attorney for the Disability Law Center. Arlene Germain, cofounder of Dignity Alliance Massachusetts, which advocates for nursing home reforms, said it is problematic that as more nursing homes establish behavioral health or other specialty units, regulations haven’t kept pace. While there are statewide standards and staffing rules for nursing homes in general, there are no state standards establishing the level of staffing and training required to run specific specialty units, like those focused on behavioral health. While the burden is on Bear Mountain to improve care, the Department of Public Health must provide robust oversight. The report found that one DPH inspection of Bear Mountain was delayed six months due to staffing constraints at DPH and inspectors lacked clinical expertise. When issues were identified, they were not always addressed. In a written response, Health and Human Services Secretary Kate Walsh said the agency is “engaged in a multi-year initiative across multiple agencies to improve quality of care in nursing facilities,” including improving screening when residents enter a home, ensuring residents have access to necessary services, and offering resources to help residents leave nursing homes. The agency is reworking MassHealth rates and conducting audits related to antipsychotic medication, Walsh wrote. The DLC report advocates for statewide licensing requirements for behavioral health units to ensure units have enough trained staff to meet residents’ needs. It suggests conditioning higher Medicaid rates for complex patients on facilities demonstrating they have adequate treatment resources. (MassHealth officials reject this approach, arguing that giving extra money to any facility with complex patients preserves consumer choice and geographic access.) The Massachusetts House in November passed a comprehensive bill aimed at improving nursing home quality. As the Senate deliberates, the Disability Law Center report provides a blueprint for additional changes that could be incorporated. Bear Mountain is not the only one-star nursing home in Massachusetts. Residents deserve better. - See the full Boston Globe editorial.
|