|
MGH Community News |
|
MGH Community News |
| December 2016 | Volume 20 • Issue 12 |
Highlights
Sections Social Service staff may direct resource questions to the Community Resource Center, Diana Tran, x6-8182. Questions, comments about the newsletter? Contact Ellen Forman, x6-5807. |
Baker Slashes Budget
Governor Charlie Baker this month unilaterally slashed $98 million from the state budget to remedy what his administration says is a gap between projected revenue and authorized spending. The total budget is $39 billion Cuts will touch a wide swath of government programs. They include health care for the poor, suicide prevention, literacy programs, and the Bureau of Substance Abuse Services. The move immediately drew blowback from the Democratic-controlled Legislature. House Speaker Robert A. DeLeo said the cuts are “premature,” as tax revenues are about on track with expectations. (As of November, they were 0.2 percent below projections.) “It seems that the administration is seeking to achieve policy objectives that have previously been rejected by the Legislature through its unilateral use of 9C cuts,” DeLeo said, referring to the section of law that gives Baker the authority to make cuts without lawmakers’ sign-off when revenues are thought to be insufficient to meet expenditures. “Recent revenue numbers indicate a need to be vigilant; they do not, however, necessitate cuts at this time.” Baker vetoed $265 million when he signed the budget in July. But the Legislature restored $231 million of that spending by overriding many of his vetoes. Many of the 9C cuts were items Baker had vetoed during the summer. Senator Karen E. Spilka, an Ashland Democrat who is the chamber’s budget chief, said Baker’s cuts will have real consequences for cities and towns struggling with opioid addiction and housing. “Governor Baker’s action...cuts important programs, including approximately $6 million in reductions to homelessness and housing, $1.9 million in cuts to substance abuse prevention programming, $900,000 in cuts to HIV/AIDS prevention and treatment services, and $400,000 in cuts to services for terminally ill children,” she said. Other affected programs include senior care. a postpartum depression pilot program (eliminated entirely), a Down Syndrome clinic and a suicide prevention account. Some of the largest cuts came from MassHealth fee-for-service payments. |
The Mass. Coalition for the Homeless elaborated on the impact these will have on housing-related services:
House Speaker Robert DeLeo says he'll try to restore funding cut by Gov. Charlie Baker yesterday when the governor unilaterally slashed state spending. DeLeo told WGBH News he expects to pass a supplemental budget in January or February that will restore at least some of the $98 million dollars Baker cut from the state budget Tuesday. DeLeo said he'll work with his Ways and Means Committee to determine if the state takes in enough revenue in December to allow spending on the cut items. DeLeo said he will focus on restoring funds for substance addiction treatment, suicide prevention, and homelessness programs that suffered from the cuts. Sources and for More Information:
Baker Administration Accused of Denying Shelter to Homeless Mothers Governor Charlie Baker’s longstanding push to end the practice of putting homeless families in motels at state expense has resulted in Massachusetts illegally denying shelter to the Commonwealth’s most vulnerable, a lawsuit from five mothers struggling with homelessness alleges. Homeless parents and children who are legally entitled to immediate accommodations are turned away because shelters are full and the state has stopped using motels as housing of last resort, the lawsuit says. As a result, the suit says, children end up sleeping in places not meant for human habitation, such as emergency rooms. Implicit in the legal action is a more pernicious allegation, one the administration strongly denies: That in service to a pledge made during Baker’s political campaign, the state is hurting residents who most need help. “By not immediately placing families who are eligible or who appear to be eligible,” the suit alleges, the state “is seeking unlawfully to reduce the demand for shelter placements, which in turn enables the agency to assert that there is no longer a need for motel placements.” The Baker administration rejected the premise of the lawsuit and strongly defended its record. “The administration is proud of its record rehousing and resheltering thousands of homeless children, reducing the number of families sheltered in motel rooms from 1,500 to under 160,” Paul McMorrow, a spokesman for the Department of Housing and Community Development, said Thursday. “Massachusetts is the only state in the nation that offers homeless children a right to shelter, and DHCD has consistently upheld that right, and acted in compliance with the law, while substantially reducing the state’s reliance on motel shelters,” he said in an e-mail. Advocates for the homeless, policy makers of both parties, and the Baker administration broadly concur that hotels and motels are often a dreadfully inadequate option for housing families. That type of lodging frequently separates them from the social support of relatives and friends, familiar schools, a clean place for children to play, easy access to public transportation, and kitchen equipment such as a refrigerator and stove. But some advocates say the administration has been too aggressive in reducing motel use. The Suffolk Superior Court suit, filed by Greater Boston Legal Services, seeks to be certified as a class action, representing all families in the state’s emergency shelter system, or eligible for it. It also contends that when the administration does provide shelter for families, the housing sometimes does not meet legal standards for being close to their hometowns and schools, or accommodating their disabilities. -See the full Boston Globe article.
Bias Incident Hotline- For Witnesses Too; Multi-Language Flyers As reported last month, the Massachusetts Attorney General's Office has launched a hotline for reporting bias-motivated threats, harassment, intimidation or violence because. New marketing materials also encourage witnesses to report. Flyers are available in Arabic, Spanish, Portuguese, and English. If you have seen or experienced a hate crime, call and report at 1-800-994-3228. For more information see the AGO website: http://www.mass.gov/ago/consumer-resources/your-rights/civil-rights/hate-crimes.html -Adapted from: Report Hate Crimes in MA: Call the Hotline!, Mass Immigrant and Refugee Advocacy Coalition e-mail, December 19, 2016. 
Changes to Education Transportation for Homeless Children- McKinney-Vento Act A Community Resource Center staff person recently attended the MA Coalition for the Homeless Housing and Benefits Meeting where Sarah Slautterback, Homeless Education State Coordinator, presented changes to the McKinney Vento Act Guidelines. The McKinney-Vento Act is federal law ensuring students experiencing homelessness have equal access to the same free and appropriate public education provided to other students. It outlines the rights of homeless students and requires collaboration and coordination across school districts and community agencies to support students. The McKinney Vento Act has recently been reauthorized to ensure procedures are implemented to identify and remove barriers preventing homeless youth from receiving educational services for which they are eligible. The following changes were effective 12/10/2016:
Additional Sources and for More Information:
Get Utilities Turned On at New Address with an Outstanding Balance from an Old Address - Cromwell Waivers We know that many of our patients and families with low-income may fall behind on their bills and may move frequently. Utility companies have the right to refuse service to someone applying for service at a new address if that person already owes for service at a previous address. They will typically ask for at least half, or the full amount, to be paid before setting up a new account. Advocacy tip: the customer has a legal right to set up a new account if
If the customer did go two or more months without paying a bill then they can ask for a “Cromwell Waiver” agreement to start new service. Basically you must
Background In the case Cromwell v. Boston Edison Company (1974) the court ruled that a company cannot shut-off service at a new address if the company learns after the fact that the person owes them money from a prior address. So companies are now very careful to screen prospective customers to avoid this scenario. Companies however can be required to enter into a so-called “Cromwell waiver” with the prospective customer. By signing a Cromwell waiver the customer is basically saying to the company, “You can add that bill from my prior address onto the bills I’ll be getting at my new address, and if I don’t pay my bill (including the bill from my prior address), you can shut off the service at my new address.” This protects the company and makes it more likely that the company will collect the old bill and so they are willing to start new service. If the company and the customer sign the Cromwell waiver, the customer then can try to negotiate a payment plan on the old bill, rather than having to pay 100% of the bill as a condition of getting service. Note that many customer service representatives are not familiar with Cromwell waivers, and will insist on getting 100% of the old bill paid before agreeing to start the new account. If that happens ask to speak with a supervisor or if that fails call the Department of Public Utilities’ (DPU) Consumer Division - 617-737-2836or toll free at 877-886-5066. -Above adapted from:
Cromwell Waivers and Shut-Off Protections National Consumer Law Center (NCLC) recently asked DPU to confirm their policy about how protections from termination apply after a customer has signed a Cromwell waiver and agreed to pay for a past balance due from a previous address. This would apply to a customer who had a past-due balance at one address, moved to another address, signed the Cromwell waiver to get service at the new address, and still has service at the new address, but now needs one of the shut-off protections. DPU's position is that if the customer is entitled to a shutoff protection, then the protection applies and the customer will not be terminated even if there is a balance from an old address and a Cromwell waiver on file. There is nothing in writing, but that is their policy. -This section from Utility Network listserv, on behalf of Jenifer Bosco, Staff Attorney, NCLC, December 01, 2016.
Massachusetts CARE Act Becomes Law The Caregiver Advise, Record, Enable (CARE) Act was signed into law by Governor Charles Baker this month. The CARE Act (pdf) recognizes the critical role family caregivers play in keeping their loved ones at home, and out of costly institutions. In 2015 in Massachusetts, family caregivers provided 786 million hours of unpaid care valued at approximately $11.6 billion annually. Lynn Nicholas, President and CEO, Massachusetts Health & Hospital Association (MHA) said, “MHA thanks AARP for working so closely with us on the development of this language. The hospital community is closely focused on keeping people healthy – both within and outside of their walls. This bill will help ensure that designated caregivers have the information they need to best support their family members and friends once they have left the hospital.” The law features three important provisions related to the family caregiver’s role when their loved one is hospitalized:
-See the full AARP announcement.
New Fact-Sheet – Recently Revised Nursing Home Regulations As reported previously (Nursing Home Regulations Revised, MGH Community News, October, 2016) the federal government issued revised nursing facility regulations in September, and most provisions became effective on November 28. The regulations are the product of over four years of work by the Centers for Medicare & Medicaid Services, including significant modifications in response to public comments received in mid-2015. -Adapted from Revised Nursing Facility Regulations are Vital, Justice In Aging e-mail, December 19, 2016.
One-Time Special Enrollment Period for Those Who Did Not Take Medicare B Thinking They Could Get Marketplace Subsidy Article amended with new information- July 2018. Many people newly eligible for Medicare thought it would be cheaper to remain in the Marketplace with subsidies, rather than pay Part B premiums, but did not realize that their Medicare Part A eligibility made them ineligible for premium subsidies, also called Advance Premium Tax Credits (APTC). When they realized their mistake, they were past their initial enrollment period and could only enroll in Part B during a General Enrollment Period, often incurring Part B late enrollment penalties. As of June 2018, CMS has now expanded this time-limited equitable relief opportunity to include people who are enrolled in Marketplace plans and could have enrolled in Medicare Part B during their Special Enrollment Period (SEP), which was available to them after they lost their or a spouse’s job-based insurance. For a limited time, these individuals can also apply for equitable relief that will give them a Special Enrollment Period to enroll in Part B. In addition, Part B late enrollment penalties will not apply. THE DEADLINE FOR APPLICATIONS IS SEPTEMBER 30, 2018. CMS has mailed notices to individuals 65 and over in this situation, advising them to drop Marketplace coverage and enroll in Part B instead. But, SSA and CMS are not publicizing this equitable relief opportunity and it is not discussed in the notice, so advocates need to get the word out.
Individuals should apply if they had any confusion and misunderstanding about the availability of tax credits or how their Medicare eligibility affected them. To request this assistance, individuals can:
-Adapted from March 31: Medicare Part B Special Enrollment Deadline, Justice in Aging e-mail, December 14, 2016.
Winter Jackets for Kids in Needs- Samaritan Steps A Community Resource staff person recently attended the MA Coalition for the Homeless Housing and Benefits Meeting where Kevin Lilly, Director of Samaritan Steps, presented about their program. Samaritan Steps works to empower and support youth, veterans, and the community in becoming self-sufficient.
Samaritan Steps is currently providing winter jackets for children of all ages, as available. Contact: 617-894-5421 or samaritansteps@gmail.com For more information about their other programs, please see their website: http://samaritanssteps.com/.
Boston Cancer Support Offers Transporation via Lyft Boston Cancer Support in partnership with the ride-hailing service Lyft is now offering a special cancer treatment transport program. Serving Boston and its surrounding neighborhoods, new users can receive a code good for 5 rides, up to $10 each. Riders are responsible for any remaining balance over the initial $10; estimates are available through the Lyft app. Riders may be able to receive additional rides on a case-by-case basis as funding allows. Rides can be used for cancer treatment, pre-screenings, and support groups Questions? Please e mail : Susan Chaityn Lebovits, Executive Director at Susan@BostonCancerSupport.org To apply: log on to request services through the website http://www.bostoncancersupport.org/lyft/ or download the Lyft App. -Thanks to Lynn Mazur for bringing this to our attention.
Crowd-Lending Agency - Axuda The DCU Federal Credit Union has launched a new small loan program called Axuda. Axuda is a non-profit working to provide small, short-term interest-free loans to individuals and families that need a helping hand. Axuda provides a forum for Borrowers to tell their stories and have their loan request crowdlended by several Axuda Lenders. Once an Axuda loan is repaid, the funds are used again to lend to other Axuda Borrowers. How it Works
To learn more visit the website https://www.axuda.org/ -Adapted from the Axuda website and Axuda - People Helping People, Massachusetts Coalition for the Homeless, December 15, 2016.
MassHealth Accountable Care Organization Pilot Details The recent MassHealth All-Provider Bulletin 262 provides additional detail on the current Accountable Care Organization (ACO) pilot. Excerpts below. Background Starting December 1, 2016, MassHealth will initiate a one-year ACO Pilot program. The program will be comprised of primary care provider-based Pilot ACOs. These ACOs will coordinate care and be accountable for the total cost of care for their attributed members within MassHealth’s Primary Care Clinician Plan (PCC) Plan. The experience of these Pilot ACOs will enable MassHealth to
With this information, MassHealth will be better prepared for the full ACO implementation anticipated in December 2017. Please visit www.mass.gov/hhs/masshealth-innovations for details and updates regarding MassHealth’s ACO program and other MassHealth innovation initiatives. Selected Pilot ACOs As a result of a competitive procurement process, MassHealth has contracted with the following six organizations to participate in the ACO Pilot program starting December 1, 2016 (please refer to the end of the bulletin for a list of participating providers within each ACO):
Primary Care Provider Billing Pilot ACOs will not be responsible for directly paying for covered services. PCCs that participate in Pilot ACOs will continue to bill MassHealth and be paid fee-for-service, as they are currently in the PCC Plan. At the end of the ACO Pilot, MassHealth will conduct a retrospective reconciliation to compare total actual costs of care for each Pilot ACO’s panel of attributed members against total expected costs for each ACO. The Pilot ACOs will share in the savings or losses with MassHealth. Non-Primary Care Providers Behavioral Health Services and ACO Referral Circles Pilot ACOs will not be responsible for contracting with a provider network. Members attributed to Pilot ACOs will continue to have access to the full MassHealth provider network of specialists, as they currently do through the PCC Plan. Members attributed to a Pilot ACO will continue to be enrolled in the Massachusetts Behavioral Health Partnership (MBHP) and receive behavioral health services through that network. Pilot ACOs may identify a list of additional providers of various provider types, with which the ACO has a special relationship. These providers can be included in what is referred to as the ACO’s “referral circle.” The PCC Plan will not require referrals for services provided to ACO-attributed members by providers within the referral circle of the member’s ACO. Referral circles are an optional component of the ACO Pilot model. Pilot ACOs may or may not choose to establish referral circles. Unless part of the ACO’s referral circle, specialists must continue to comply with the PCC Plan’s referral requirements for services rendered to PCC Plan enrollees. For more information regarding the PCC Plan’s referral requirements, please refer to 130 CMR 450.118: Primary Care Clinician (PCC) Plan. Member Attribution and Notification PCC Plan members whose PCC is participating with a Pilot ACO will be attributed to that Pilot ACO. MassHealth will notify PCC Plan members whose PCC is participating in a Pilot ACO. Members will be notified of their ACO attribution prior to December 1, 2016. Members who do not want to participate in the Pilot ACO may choose another PCC that is not participating in a Pilot ACO at any time. Members should ensure that the PCC they are currently assigned to is the PCC they see for primary care services. If a member receives most primary care services from someone other than their assigned PCC, they should contact MassHealth to change PCCs. Members can change their PCC by contacting the MassHealth Customer Service Center at 1-800-841-2900 or visiting www.mass.gov/masshealth (click the “MassHealth Members and Applicants” button on the left and then click the “Enroll in a Health Plan” link). Additional Information Additional information on MassHealth’s planned restructuring and payment reforms may be found on the MassHealth Innovations website at www.mass.gov/hhs/masshealth-innovations. -See the full bulletin at http://www.mass.gov/eohhs/docs/masshealth/bull-2016/all-262.pdf
MassHealth enrollment is at 1.9 million and continues to grow. MassHealth has announced a series of initiatives designed to prune the rolls of people who may not be eligible. Unfortunately, the pruning is likely to also affect individuals who remain eligible, but missed paperwork deadlines or got caught up in systems defects. Be on the lookout for clients and patients coming in with termination notices or notices requesting information by a deadline. Remember MassHealth beneficiaries can stop an erroneous termination if they appeal before the date scheduled for termination. Important Numbers and Dates
-From December MassHealth Update, Health Announce listserv, on behalf of Vicky Pulos, Mass Law Reform Institute, December 19, 2016.
MassHealth Managed Care – First Fixed Enrollment Period Begins Jan 1, 2017 As reported previously (MassHealth Managed Care Organization (MCO) Lock-In and Primary Care Clinician (PCC) New Referral Requirements, MGH Community News, September, 2016), MassHealth has instituted a MCO lock-in that limits when members can change plans. The first Fixed Enrollment Period begins January 1, 2017 for people who were enrolled in mandatory managed care on October 1, 2016. MCO members who want to change plans will have to call MassHealth and show one of 11 permissible reasons (below) to change plans during their Fixed Enrollment Periods. Denial of a request to change plans is appealable. New applicants will have 90 days from managed care enrollment to freely change plans before they are locked in for the year.
If you are in a Fixed Enrollment Period, you may request to change your health plan if one of the following reasons applies to you:
MassHealth will send you a letter at the start of your Fixed Enrollment Period that gives you more information. More information at http://www.mass.gov/eohhs/gov/departments/masshealth/important-changes-for-members-of-mco-and-pcc-plans.html -Adapted from December MassHealth Update, Health Announce listserv, on behalf of Vicky Pulos, Mass Law Reform Institute, December 19, 2016, with additional material from the mass.gov website.
Hospital Observation Status - the Impact on Patients Many Medicare-covered hospital patients may no be aware that they are under Observation Status. One problem with this is that if they then go to a skilled nursing facility for follow-up care they aren’t covered by Medicare and have to pay out-of-pocket, but there are additional costs for patients as well. The Center for Medicare Advocacy has developed a very useful infographic explaining this practice and steps patients and their family members can take in response. What is “Outpatient” Observation Status? Observation status is a billing code hospitals use to protect from overzealous auditors and Medicare readmission penalties. This may be called “outpatient,” but it has nothing to do with where a patient receives care or the kind of care received. It may just seem like semantics, but for Medicare beneficiaries, the consequences can be very real. Under Observation Status patients are responsible for increased out-of-pocket expenses. Patients who don't have Medicare Part B are responsible for the FULL COST of the hospitalization and may be responsible for the cost of prescriptions that would be covered if they were admitted to the hospital. Nursing home care- patients, with some limited exceptions, must be classified as inpatients for 3 days in the hospital in order for Medicare to pay for subsequent nursing home care. If post-hospital care in a nursing home won’t be covered by Medicare, many people Medicare Advocacy is starting an “Ask About Observation Status!” educational campaign.
San Antonio as Model of Mental Health Care - Globe Spotlight Team The San Antonio Police Department’s seven-person mental health unit is just one piece of a larger behavioral health care system in San Antonio and surrounding Bexar County that’s widely considered to be a national model. Over the past decade and a half, San Antonio community leaders, government officials, law enforcement, judges, medical institutions, and the county mental health authority have made tremendous strides together in identifying and treating people with mental illness. They’ve taken on many of the critical problems this Spotlight series has found still rampant in Massachusetts, including poor coordination among institutions, limited training for law enforcement, and dwindling options for care. They have acted aggressively and spent heavily, confident their investments would pay off. They’ve done what many Bay State advocates dream of, and one thing those advocates resist: taking decisions on treatment and medication out of the hands of the most severely ill. This coalition in San Antonio has built a crisis center for psychiatric and substance abuse emergencies and a 22-acre campus for the homeless that resembles a community college. To date, more than 100,000 people have been diverted from jail and emergency rooms to treatment, local officials say, resulting in a savings of nearly $100 million over an eight-year period. Thousands of emergency responders in San Antonio and Bexar County have been trained to manage mental health crises. Local judges devised an involuntary outpatient treatment program for people resistant to help and special juvenile court sessions for teens struggling with mental illness. An alliance of mental health specialists set up a transitional clinic to make sure people released from hospitals have immediate access to therapy and medication. And in May, the county opened a $2 million reentry center designed in part to help mentally ill inmates transition to society. “San Antonio is still way ahead of the curve,” said Ron Manderscheid, executive director of the National Association of County Behavioral Health and Developmental Disability Directors. San Antonio’s system isn’t flawless. Tens of thousands of people still aren’t getting adequate treatment, according to the local head of the National Alliance on Mental Illness. Families have suffered tragedies as a consequence. And key changes in leadership this year and next will test the system’s resilience. But it is actually a system, and with it San Antonio is leagues ahead of most of its peers. Law enforcement, health care, and mental health officials from across the country visit and consult constantly, eager to replicate the wise investments and collaborative spirit that have saved many lives and millions of dollars. Massachusetts officials have begun paying attention, too, led by Middlesex Sheriff Peter Koutoujian, who last year began closely studying Bexar County’s success. Koutoujian plans to travel to San Antonio in January to see it for himself. Perhaps no city or state in America has completely fulfilled the promise of seamless, sterling community care that accompanied deinstitutionalization of people with mental illness. But the vanguard lies here in San Antonio, an oasis of creativity and dedication in a state not known for progressive social policy. -See the full Boston Globe Spotlight Team article.
21st Century Cures Act - Analysis Congress passed sweeping legislation this month that boosts funding for medical research, eases the development and approval of experimental treatments and reforms federal policy on mental health care. The 21st Century Cures Act provides for $4.8 billion in new funding for the National Institutes of Health; of that, $1.8 billion is reserved for the “cancer moonshot” launched by Vice President Biden to accelerate research in that field. Another $1.6 billion is earmarked for brain diseases including Alzheimer’s. Also included are $500 million in new funding for the Food and Drug Administration and $1 billion in grants to help states deal with opioid abuse. The bill, however, had vocal progressive critics — Sens. Bernie Sanders (I-Vt.) and Elizabeth Warren (D-Mass.) prime among them — who said the bill’s changes to drug approval processes gave too many concessions to pharmaceutical companies. Public Citizen, a progressive activist group that opposed the bill, called it “sorely disappointing that Congress gave Big Pharma and the medical device industry an early Christmas present” that “comes at the expense of patient safety by undermining requirements for ensuring safe and effective medications and medical devices.” Here are some of the winners and losers in the 21st Century Cures Act: Winners Pharmaceutical and Medical Device Companies. The bill will likely save drug and device companies billions of dollars bringing products to market by giving the Food and Drug Administration new authority and tools to demand fewer studies from those companies and speed up approvals. Medical schools, hospitals and physicians. The bill provides $4.8 billion over 10 years in additional funding to National Institutes of Health, the federal government’s main biomedical research organization. (The funds are not guaranteed, however, and will be subject to annual appropriations.) The money could help researchers at universities and medical centers get hundreds of millions more dollars in research grants, most of it toward research on cancer, neurobiology and genetic medicine. Mental health and substance abuse advocates. The bill provides $1 billion in state grants over two years to address opioid abuse and addiction. While most of that money goes to treatment facilities, some will fund research. The bill also boosts funding for mental health research and treatment, with hundreds of millions of dollars authorized for dozens of existing and new programs. Patient groups. Specialty disease and patient advocacy groups supported the legislation and lobbied vigorously. Many of these groups get a portion of their funding from drug and device companies. The bill includes more patient input in the drug development and approval process, and the bill is a boost to the clout of such groups. Health information technology and software companies. The bill pushes federal agencies and health providers nationwide to use electronic health records systems and to collect data to enhance research and treatment. Although it doesn’t specifically fund the effort, IT and data management companies could gain millions of dollars in new business. Losers Preventive medicine. The bill cuts $3.5 billion — about 30 percent — from the Prevention and Public Health Fund established under Obamacare to promote prevention of Alzheimer’s disease, hospital acquired infections, chronic illnesses and other ailments. Consumer and patient safety groups. Groups like Public Citizen and the National Center for Health Research either fought the law outright or sought substantial changes. Although they won on some points, these groups still say Cures opens the door for unsafe drug and device approvals and doesn’t address rising drug costs. The FDA. The bill gives the FDA an additional $500 million through 2026 and more hiring power, but critics say it isn’t enough to cover the additional workload under the bill. The agency also got something it opposed: renewal of a controversial voucher program that awards companies that approve drugs for rare pediatric diseases. Special Needs Trusts One small, easily overlooked provision has changed a law dating back to 1993. Back then, Congress authorized the creation of so-called (d)(4)(A) trusts which permit people with disabilities under age 65 to shelter funds and still qualify for Medicaid (MassHealth in Massachusetts) and Supplemental Security Income. The law has required these trusts to be created by a parent, grandparent, guardian or court, even if the beneficiary is competent to create the trust herself. This has limited the availability of these trusts and required expensive proceedings in court which have often delayed eligibility for vital public benefits. Finally, due to the advocacy of the National Academy of Elder Law Attorneys, Congress has acted to correct the mistake. Learn more about (d)(4)(A) trusts. Criticism “The problem with bills in Congress that roar toward passage like juggernauts is that they’re especially worthy of close examination, and especially unlikely to get it. That’s the story with the 21st Century Cures Act.” said Michael Hiltzik in an LA Times column, excerpted here: The 21st Century Cures Act is a huge deregulatory giveaway to the pharmaceutical and medical device industry, papered over by new funding for those research initiatives. The punchline is that the regulatory rollback is real, but the funding may not be — it’s subject over the next decade to annual appropriations by Congress that might never come. “This continues a trend of eroding standards at the Food and Drug Administration since the 1990s,” says Michael Carome, director of the Health Research Group at the advocacy organization Public Citizen, which issued a broadside against the bill last month. “We don’t think there should be any further erosion.” Moreover, despite the universal praise for provisions for state grants to battle opioid abuse and for mental health research and treatment, it also cuts $3.5 billion, or about 30%, from Obamacare’s Prevention and Public Health Fund, which fosters work to prevent Alzheimer's disease, hospital-acquired infections and other conditions, according to Kaiser Health News. One would expect Congress to ask the drug industry for something in return for regulatory rollbacks of this magnitude. Remarkably, nothing in the measure would address the main problem the public sees with the drug industry — inordinately high prices. The bill opens a path for the FDA to approve new uses, or indications, for existing drugs without demanding thorough clinical tests conducted along customary lines. These include randomized samples, to prove they’re safe and effective for the new indications. Instead, the FDA could rely on “real world evidence,” which includes observations, safety and side-effect claims, and other data not subject to rigorous analysis. “That’s a much lower level of evidence,” Carome says. "A homeopath would love this provision, and, I’m sure, so would drug companies," David Gorski, an oncologist and prominent debunker of pseudoscience and medical nostrums, wrote last year. "Why bother with the time, bother and expense of those pesky clinical trials to get your drug approved for additional indications, when you can rely on clinical experiences?” "The bill also allows drug makers to promote off-label uses of their drugs to insurance companies. This would allow them to vastly expand the markets for these drugs while bypassing FDA scrutiny. And it creates what Public Citizen calls an “overly broad” category of “breakthrough devices” that the FDA will be pressured to approve hastily. These rollbacks are premised on the notion that the FDA has been a bottleneck in drug and device approval. As we reported earlier, the libertarian right loves to attack the agency for its careful approach to drug approval, even blaming it for killing people denied ostensibly lifesaving drugs. In fact, the FDA often performs more like a rubber stamp for Big Pharma than a bottleneck: Last year, the FDA approved 89% of applications for new drug uses, according to three experts writing at Health Affairs. The possibility of harm from overly indulgent regulatory approval is conveniently overlooked by industry mouthpieces demanding lessened scrutiny. Consider Merck’s Vioxx, a painkiller and arthritis drug the FDA approved in 1999. Vioxx was pulled off the market in 2004 after it was shown to raise the risk of heart attacks. By then, according to research in the British medical journal Lancet, 88,000 Americans had heart attacks from taking Vioxx, 38,000 of them fatally. Carome further points to the case of Essure, a device implanted in women’s fallopian tubes as an alternative to permanent surgical sterilization. Currently marketed by Bayer, Essure was given expedited approval by the FDA in 2002 based on “two nonrandomized, nonblinded, prospective studies that lacked a [control] group and enrolled a total of 926 women,” according to a report last year in the New England Journal of Medicine. Experience since then has pointed to serious potential side effects and a lack of firm evidence that the device is safer than tubal ligations, amid signs it may be less effective at preventing pregnancy. The FDA hasn’t taken Essure off the market, but it has convened a new study panel and requires a stringent warning of health risks on the label. Sources and For More Information
- The Washington Post
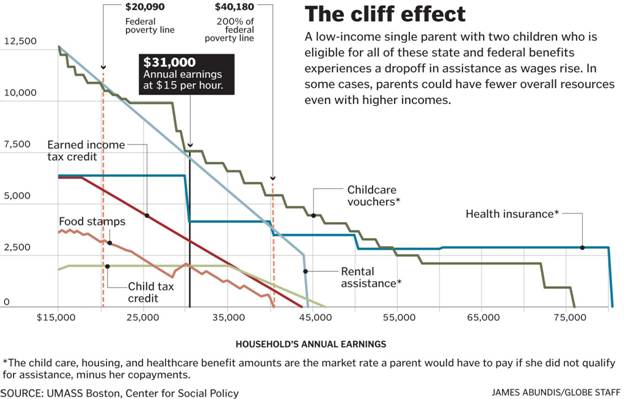
$15 minimum wage could squeeze workers on public assistance If it succeeds, a campaign to raise the Massachusetts minimum wage to $15 an hour could put more money in the pockets of low-income workers and create a path to self-sufficiency. But for some families, the boost in pay could mean a drop of hundreds of dollars a month in government benefits. Food stamps, child care vouchers, and rent subsidies could be cut before families can afford to cover those expenses on their own, leaving some households, particularly single parents with young children, worse off despite a bigger paycheck - a phenomenon known as the “cliff effect.” A single parent with a 3-year-old and an 8-year-old living in Boston who works full time and receives multiple public benefits, for instance, would see her overall resources drop at the $15-an-hour mark and be no better off until her wages climbed above $24 an hour, according to an analysis by the Center for Social Policy at the University of Massachusetts Boston. Being in this zone, where wages are too high for significant assistance but not high enough to survive, can cause people to turn down raises or extra hours in order to hold on to taxpayer-funded benefits that can be more valuable than a small increase in pay. “This is a group of people who did exactly what they were told: They’re working,” said Randy Albelda, the UMass-Boston economics professor who conducted the cliff effect analysis. “They find pretty quickly, when I get a raise or my manager wants me to work more hours, uh-oh, I might lose my health care.” President-elect Donald Trump recently named Andrew Puzder as his nominee for labor secretary, a move that could energize opponents of boosting the federal minimum wage. In a 2015 op-ed on the political website The Hill, Puzder, chief executive of the company that owns the Carl’s Jr. and Hardee’s restaurant chains, railed against minimum wage increases, arguing that “people get trapped into working less and keeping valuable benefits over working more and losing them.” Instead, he favors expanding the earned income tax credit. States are free to raise wages independently, and a coalition of workers’ advocates in Massachusetts is in the process of drafting legislation to raise the state minimum to $15. Nearly 100,000 single-parent households in Massachusetts could be affected by a raise to $15 an hour, according to the Economic Policy Institute in Washington, D.C. Most will end up with more assets, despite a loss of benefits, but some will fall over the cliff. The problem lies in the way the benefits systems were set up decades ago — to help people who didn’t work, including single mothers and people with disabilities. As a result, the rising incomes of today’s benefits recipients weren’t properly accounted for, nor was the cost of child care, and some assistance programs max out before workers can get to a level where they can survive on their own. Many benefits are also tied to the federal poverty level, which is based on food costs; it doesn’t account for expenses such as housing that have grown disproportionately and does not factor in regional cost of living differences. There have been attempts to help people whose benefits are slashed as their incomes rise. Earlier this month, the Department of Transitional Assistance, which administers cash payments and food stamps, started offering a gradually decreasing four-month stipend for low-income workers whose earnings make them ineligible for assistance. The department also recently modified how it calculates clients’ income in order to give them more assistance. Workers’ advocates who support raising the minimum wage to $15 an hour say that now is the time — before wages potentially rise — to reexamine the outdated approach to administering benefits. If it isn’t overhauled, they worry that the cliff effect could become a rallying cry for those who oppose increasing the minimum wage. “I think what’s going to happen is employers might say, ‘We can’t go to $15 an hour because of the cliff effect,’ ” said Albelda, the UMass professor. “Or [House Speaker] Paul Ryan will say that. So I think a lot of advocates now want to say it’s not a problem or say it’s not true.” “It’s not the problem of the minimum wage,” she added. “It’s really a problem with how we think about combining employment with public support.”
-See the full Boston Globe article.
How to Persuade the Public to Care About Other People's Problems When trying to win support for an antipoverty program like welfare, it's not what you're saying that's most important, it's how you're saying it. At least according to a study by the FrameWorks Institute, a nonprofit research organization focused on the communication of ideas in social policy. Nat Kendall-Taylor, FrameWorks' CEO, says that many officials in human services don’t think of themselves as messengers who can shape the way the public perceives and responds to social problems. But they should. By embracing their communications role and making intentional decisions about messaging, Kendall-Taylor argues officials can do a better job promoting the most effective policy solutions. Frames matter. The way you talk about your issue can have a significant impact on the way people think and what they do. Take the expert saying something about the negative health and educational effects of early, chronic, severe stress on a child’s development. Stress is the frame. It is the thing that activates cultural models that people then use to come up with an understanding of the information they're receiving. A very dominant way that Americans have of thinking about stress is this boot straps/John Wayne sense of “what doesn’t kill us makes us stronger.” People tend to think that stress is actually something that kids need to develop grit, fortitude, drive, will power and gumption. That frame of stress, without additional strategies, generates an understanding that is almost directly in opposition to the intention of the message. I could easily fill a blog on poverty with examples and statistics that make it clear that this is a really bad problem. But if it is all about the problem, just leaving someone there doesn’t get someone to think in new ways about the issue. It gets people to shut down. Even saying, “it’s a cycle of poverty,” and not ending there, but saying, “that can be broken if we…” and saying a couple of general things is better. Giving people cognitive cues that there are solutions that are possible makes for a really different takeaway. Kendall-Taylor also warned against “myth-busting”. If I am a public official, and I’m hearing distressing falsehoods about one of my programs, how do I make sure that people absorb the correct information and stop listening to falsehoods? Start with the position that you’re trying to advance. When it comes to issues of framing, the order really matters. The problem with myth-busting in general is that people start with the myth and remind people of the misperception, giving it a chance to expand and gain momentum. And then they discredit it with a more logical truth. Unfortunately, cognition is not logical in that way. Instead, if you lead with the thing that you are trying to get people to believe, and you do a good job of cementing it in their thinking, there is a point in a message where you can correct the misperception. -See the full Governing article.
Data on Boston Evictions Lacking As Boston officials ramp up efforts to combat evictions, they’re running into a problem: No one really knows how many evictions there are. City officials and housing advocates have long complained there is no comprehensive data on evictions collected in Boston; what few numbers that are available usually come from contested evictions that end up in Housing Court. And even getting those requires an arduous counting of individual cases. The results are usually old and incomplete. Moreover, those figures vastly undercount the extent of displacement in the city, since most evictions don’t even end up in court. So while rising rents and anecdotes of mass evictions from fast-changing neighborhoods such as East Boston have pushed displacement to the fore of the city’s agenda, there’s no clear way to measure just how much of a problem this has become. In a City Hall that is increasingly data-driven, that has become a frustrating challenge. In legislation he filed earlier in December to add protections for renters, Mayor Martin Walsh also proposed requiring landlords to notify the city when they move to evict a tenant. That will give officials a paper trail to document eviction activity in real-time. “We want to get information as it’s happening, so we can reach out to people and get tenants the help they need,” said Sheila Dillon, Boston’s housing chief. “We can use that data in all sorts of ways.” The data could be used to pinpoint eviction hotspots, allowing city officials to direct counseling resources, and also help them understand what may be causing evictions and how they might be addressed. Walsh has also created a new Office of Housing Stability, which would use the notices filed by landlords to provide tenants facing eviction with information about their rights and counseling resources. Such interventions may head off more evictions before they start, said Lydia Edwards, who heads up the new office. “About 80 percent of evictions are people who don’t ever go to court,” Edwards said. “We’d be able to finally know about all of these people and get them information to help.” -See the full Boston Globe article.
Medicare Isn’t Going Bankrupt House Speaker Paul Ryan is repeating a myth that The Center on Budget and Policy Priorities (CBPP) and others have debunked before: that Medicare is running out of money. “Medicare goes bankrupt in about 10 years,” he said on CBS’ “60 Minutes,” adding that “for the X-Generation on down, it won’t be there for us on its current path.” That’s just not true. Medicare’s Hospital Insurance (HI) trust fund will remain solvent - that is, able to pay 100 percent of the costs of the hospital insurance coverage it provides - through 2028, the program’s trustees wrote in their latest report. Even after 2028, when the HI trust fund is projected for depletion, incoming payroll taxes and other revenue will still cover 87 percent of Medicare hospital insurance costs. Policymakers will need to close this shortfall by raising revenues, slowing the growth in costs, or most likely both, as they’ve done many times before. But Medicare’s hospital insurance program will not run out of all financial resources and cease to operate after 2028, as “bankruptcy” suggests. Contrary to Ryan’s widely discredited claim last month that the Affordable Care Act weakened Medicare’s finances, health reform (along with other factors) has significantly improved Medicare’s financial outlook, boosting revenues and making the program more efficient. The trustees now project that the HI trust fund will remain solvent 11 years longer than before health reform was enacted. And the HI program’s projected 75-year shortfall of 0.73 percent of taxable payroll is much less than the 3.88 percent of payroll that the trustees estimated before health reform. (See chart below.)
This means that policymakers could close the projected funding gap by raising the Medicare payroll tax — now 1.45 percent each for employers and employees — to about 1.8 percent, or by enacting an equivalent mix of program cuts and tax increases. The 2028 date doesn’t apply to Medicare coverage for physician and outpatient costs or to the Medicare prescription drug benefit, neither of which faces insolvency. They’re financed through the program’s Supplementary Medical Insurance (SMI) trust fund, which consists of two separate accounts — one for Medicare Part B, which pays for physician and other outpatient health services, and one for Part D, which pays for outpatient prescription drugs. Premiums for Part B and Part D are set each year at levels that cover about 25 percent of costs; general revenues pay the remaining 75 percent. Therefore, SMI can’t run short of funds. -See the original CBPP blog post.
New Brief Finds 30 Million Would Lose Coverage under Past ACA Repeal Plan This month, the Urban Institute (the Institute) released a brief discussing the impact of enacting the same partial repeal of the Affordable Care Act (ACA) advanced by Congressional Republicans in 2016. This repeal (H.R. 3762), using the legislative reconciliation tool, was vetoed by President Obama, but it is widely believed that President-Elect Trump would be likely to sign an identical bill. Other estimates account for all of the people who gained health insurance coverage through the ACA, approximately 22 million people through the combination of the Medicaid Expansion and the individual Marketplace. But in this brief, the Institute delves deeper into the mechanisms of the individual insurance market to find that nearly 30 million people would be without meaningful health care coverage if Congress passed this same bill again. This would not be a reversion to pre-ACA levels, but an increase in the uninsured because of damage to the markets. The partial repeal would damage the individual insurance markets by retaining the rules for insurers without, in turn, requiring individuals to purchase coverage. Insurers would still be required to cover pre-existing conditions, to guarantee issue, and not to base premiums on health status, sex, or age beyond a mandated formula. But individuals would be able to leave the market at any time and return without penalty if and when they need health care. This combination would lead to insurers covering only an older, sicker population as younger, healthier people choose to save money and drop their insurance. Insurer costs would rise, causing them to either raise premiums or to leave the individual market entirely, potentially in the middle of the plan year. In addition, pulling the current subsidies provided by the federal government to low- and middle-income people for health care coverage would hasten the decline of the markets. Medicare Rights is deeply concerned about the implications of repealing the ACA and delaying the development of a meaningful replacement plan, and we will advocate for continued access to affordable coverage for Americans of all ages. -See the original Medicare Rights Center blog post.
|
||||||||||||||||||||||||||||||||||||||||||||||