|
MGH Community News |
|
MGH Community News |
| September 2016 | Volume 20 • Issue 9 |
Highlights
Sections Social Service staff may direct resource questions to the Community Resource Center, Lindsey Streahle, x6-8182. Questions, comments about the newsletter? Contact Ellen Forman, x6-5807. |
The MBTA Launches RIDE Pilot Program with Uber and Lyft A version of this article was e-mailed to the Social Service Department earlier this month. Gov. Baker recently announced a new year-long pilot program in which Boston area The RIDE riders can choose to get service from Uber or Lyft. If accepted into the On-Demand Paratransit Pilot Program:
How it Works
Note: Lyft customers who are unable to use or do not have access to a smartphone can use a phone-in option. Uber will provide smartphones to a limited number of eligible customers for use on a limited basis to book trips.
Both companies will now provide wheelchair-accessible vehicles, and all drivers will go through safety screenings, including criminal and vehicle background checks. (Massachusetts law recently mandated a more rigorous check for ride-share drivers). Drivers in the pilot program will attend special training sessions to improve their understanding of paratransit customers’ needs.
|
Note: The MBTA reserves the right to limit or cancel this pilot program at anytime. More information or to sign-up: http://www.mbta.com/riding_the_t/accessible_services/default.asp?id=6442456760 Press coverage/more information:
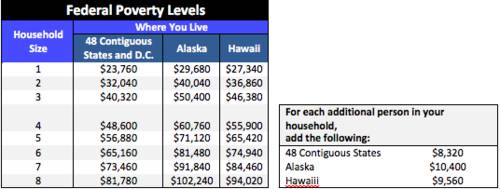
Starting October 1st, elders, people with disabilities, unaccompanied youth, and other households will be able to access up to $4,000 in RAFT funds to avoid or exit homelessness. Funds likely will run out quickly, though, as the funding for households without children under the age of 21 is capped at $500,000 statewide. Individuals and other households can apply for RAFT through their local provider. A list of providers and program criteria can be found via the Department of Housing and Community Development website. See statewide 50% Area Median Income limit. -From Kelly Turley, MA Coalition for the Homeless, September 29, 2016.
311 Now Connects Bostonians With Addiction Recovery Services People looking for help with addiction can now access city services in Boston by using the 311 system (Can't access 311? Call 617-635-4500.) While the 311 service has typically been reserved for filing complaints about potholes, parking tickets and graffiti, officials say it will now also connect people to public recovery services. Constituents will be transferred to representatives from the Boston Public Health Commission's addiction treatment and support program, PAATHS. "Even though there are so many resources in the city of Boston, not everybody knows how to access them," Brendan Little, policy director for the city's Office of Recovery Services, said. "We have police officers or teachers or various community members saying, 'I don't know how to get help for my loved one, I don't know how to get help for myself.' " An ad campaign also launched this month to help spread awareness about the additional Bos:311 service. -See the full WBUR story.
SNAP Cost of Living Changes Effective October 1st - Mixed Impact Expected SNAP Cost of Living Adjustment (COLA) changes, effective October 1, 2016, will have a mixed impact. Some will see an increase in benefits and some will see a decrease On the GOOD news front, the SNAP Shelter Deduction increases nationwide from $504 to $517/mo, and the "Standard Deduction" for 1-3 person households increases from $155 to $157/mo. These changes mean that the amount one can deduct from income is greater, resulting in a lower countable income and an increased benefit amount. On the BAD news front, the Standard Utility Allowance (SUA) for Massachusetts decreases (resulting in a benefits decrease):
The reason for the drop in the value of the SUA is because energy costs continue to decline and the SUA is based on consumer price index (CPI) of utility costs. The SUA increases and decreases are state-specific to the SUA formula, so not every state sees this level or amount of fluctuation. Based on information DTA staff shared at the Western Mass SNAP Coalition last Friday, DTA has roughly projected that the following SNAP households will experience SNAP decreases and increases:
You may hear from clients confused about the change in their SNAP. DTA is sending out a notice this week announcing the revised SNAP. You can help these individuals with claiming any out-of-pocket medical expenses or dependent care expenses (including adult dependent care) to boost their SNAP. Try to screen the individual for medical expenses and report that to DTA if these are not already claimed. For more information on SNAP medical expenses, go here: http://www.masslegalservices.org/content/food-stamps-snap-and-medical-expense-deduction -Adapted from Food/SNAP Coalition listserv, on behalf of Pat Baker, MLRI, September 26, 2016.
FAQs for Power of Attorney Agents Have you been asked to serve as an agent (or "attorney-in-fact" to use the technical term) under a durable power of attorney in Massachusetts, but you're not totally sure about your duties and responsibilities? Then you're not alone. Here's an excerpted primer. What are my duties as attorney-in-fact? If you have been appointed to represent the "principal" with respect to her financial affairs, this means that in effect you can step into her shoes and take whatever investment and spending measures the principal would take herself. Unless limitations have been placed in the power of attorney itself, you can open bank accounts, withdraw funds from bank accounts, trade stock, pay bills, cash checks. All steps you take must be consistent with your role as a "fiduciary." What does it mean to be a "fiduciary"? This means that you will be held to the highest standards of good faith, fair dealing and undivided loyalty with respect to the principal. You must always act in his best interest and keep his goals and wishes in mind in making any discretionary decision. Can I be held liable for my actions as attorney-in-fact? Yes, but only if you act with willful misconduct or gross negligence. If you do your best and keep the principal's interests in mind as the basis of your actions, you will not incur any liability. When does the power of attorney take effect? Unless the power of attorney is "springing", it takes effect as soon as it is signed by the principal. In most cases, even when the power of attorney is immediately effective, the principal does not intend for you to use it until and unless she becomes incapacitated. You should discuss this with the principal so that you know and can carry out her wishes. A "springing" power of attorney takes effect only when the event described in the instrument itself takes place. Typically, this is the incapacity of the principal as certified by one or more physicians. Conclusion Too often clients get appointed to roles that carry huge responsibilities and they are given little instruction on how to carry out their roles. Or, even if they are well advised, they cannot remember all they were told at a single meeting. The Consumer Financial Protection Bureau has published a series of easy-to-read guides on filling these fiduciary roles. These booklets can reinforce the advice given by the attorney and be available as a reference when new issues arise. Here's a link to their guide for an Agent under a durable power of attorney. Use it to your advantage! -See the full Margolis & Bloom article.
DTA to Open Quincy Office on Oct 3 DTA is opening an office in Quincy at 1515 Hancock Street. DTA had a Quincy office in the past that had closed. The coverage area will include Quincy, North Quincy, Wollaston, Dedham, Dorchester (02122/02124), Milton, Norwood, Westwood, Braintree, East Weymouth, Hingham, Hull, North Weymouth, South Weymouth, Weymouth, Cohasset, Norwell, Scituate, North Scituate and Squantum. Effective Monday, October 3, 2016, DTA clients who live in those communities will be assigned to the new Quincy Transitional Assistance Office (TAO). Note: at this time this office will NOT accept Emergency Assistance (EA) family shelter applications. Here’s a flyer that can be distributed or posted.
Final Head Start Rules for Homeless Families Announced The U.S. Department of Health and Human Services recently announced final regulations to update the Head Start Performance Standards. The regulations contain new policies on the prioritization and attendance of homeless children, as well as other procedures to facilitate the identification, enrollment, and stability of homeless children in Head Start and Early Head Start.
Download a complete summary of all of the Head Start regulations specifically related to homelessness, including citations.
Housing Panel Shares Advocacy Tips The iCMP recently hosted a housing panel and invited Community Resource Center staff to attend. Steven Farrell, Metropolitan Boston Housing Partnership (MBHP), Barbara Sheerin, Boston Housing Authority (BHA) and Elizabeth Winston, Just a Start (JAS) were the featured speakers. Here are some of the advocacy tips they shared. Waiting Lists
Applications
Program Highlights
Open Waitlist
-Thank you to the iCMP Team, Mary Neagle and host Rolando Mercado.
Homeless Families Being Moved from Hotels The number of homeless families housed in hotels statewide continues to drop as the administration of Gov. Charlie Baker pushes for an eventual end to the program which uses hotels and motels as overflow for congregate and scattered site family shelters in the Emergency Assistance (EA) program. According to Department of Housing and Community Development Undersecretary Chrystal Kornegay Baker and Lt. Gov. Karyn Polito made a campaign promise to eliminate the program by the end of their first term, and they're well on their way to meeting that goal. One of the major efforts the state undertook to eliminate the use of hotels as temporary shelters was to expand the number of state-contracted shelter beds for homeless families, Kornegay said. Those beds are in a number of settings: congregate, co-housing and individual units, she said. Some of the families leaving the hotels are sent to shelters farther than expected from their community of origin. Last month, The Sun learned of a Woburn-area family, once housed in a Chelmsford hotel, that was sent to Holyoke, a city on the other side of the state. Kornegay said this is not the norm, and the state always tries to place a family within 20 miles of its community of origin in order to minimize disruption. "We make every effort we can," she said. "Sometimes, it's just not possible." Kornegay said they're working across the system to reduce the total caseload and get families out of shelters. She said there's a greater focus on how to stabilize families before they become homeless -- including those who need help but may not be eligible for emergency assistance. The state is seeking "communities who are willing to allow the development of affordable housing, so we can create opportunities for families at all income levels," Kornegay said. Baker's 2017-2021 capital plan, released in May, set forth $1.1 billion for housing production and preservation. The funds will be used to preserve privately owned affordable housing units with expiring affordability restrictions; develop supportive housing for homeless families and the disabled; advance development of mixed-income housing and small-scale affordable housing; preserve and redevelop local public housing communities through public-private partnerships; and capital projects at state-supported public housing communities. Earlier this month, Baker announced awards of $31 million in state and federal low-income housing tax credits and $59 million in housing subsidy funds for 26 affordable housing projects across the state. Homeless families in hotels statewide:
Homeless-family population statewide as of Aug. 29:
Voting- Absentee Ballots, Early Voting and Last-Minute Requests Each presidential election the Community Resource Center fields questions from inpatients who want to cast a ballot. Ideally voters will plan ahead to avoid uncertainty at the last minute. Below adapted from/and for more information: www.sec.state.ma.us/ele/eleifv/howabs.htm Absentee Ballots Under Massachusetts law one may vote by absentee ballot if one:
Apply in writing to your city or town clerk or election commission. There is an application form available at your local election office or by downloading one of the applications below. You may also make application by letter or note. Whichever method you choose, the application must be made in writing and signed. If writing a note include:
Note: A family member of a person qualified to vote by absentee ballot may APPLY for the ballot on their behalf (but not vote on their behalf). Deadlines
Early Voting Massachusetts joined 32 other states that allow voters to cast their ballots before Election Day. In June 2014, Gov. Deval Patrick signed a package of reforms aimed at increasing voter participation. The early voting provision, which will goes into effect for general elections beginning in 2016, now allows in-person early voting up to 11 businesses days before the election. Last Minute Voting (for Inpatients) Last Minute voting - within 5 Days of the election: If a Massachusetts voter has entered a health care facility anytime after noon of the 5th day before the election, and doesn’t have anyone to pick up an absentee ballot and return the completed ballot by the deadline, contact the city or town clerk about the proper procedure to be followed. -Social Service Staff can see our Voting Rights page for more information.
Lipodystrophy Treatment Coverage is Now Law On August 10, 2016 Governor Charlie Baker signed into law An Act Relative to HIV-Associated Lipodystrophy Syndrome Treatment, which will go into effect November 9. This first-of-its-kind legislation, sponsored by Senator Mark Montigny and Representative Sarah Peake, requires public and private insurers to cover treatment of a debilitating side effect of early HIV medications. The result of tireless advocacy, including State House testimony by our own ID social worker Sandy McLaughlin, this law means that some of the longest-term survivors of the HIV epidemic will finally have access to critical health care they need and deserve. What is lipodystrophy?Lipodystrophy is a disfiguring side effect of some early HIV treatments, characterized by painful, abnormal changes in body shape, such as fat growths on the back of the neck that press on the spine, and facial wasting that is seen as a public disclosure of HIV status. Lipodystrophy causes profound and unnecessary suffering: spinal malformation and posture problems, headaches, restricted mobility, depression and anxiety, suicidality, and stigma. What does this law do?Although there are effective treatments for lipodystrophy, including liposuction and facial fillers, insurers have routinely denied claims for these services on the improper grounds that they are cosmetic. This law rectifies that problem. It requires that private insurers, MassHealth and the Group Insurance Commission (for state employees) cover medical treatments for HIV- associated lipodystrophy. What treatments for lipodystrophy are covered?The law does not place any limit on what treatments or therapies are covered. To quote the legal lingo, the law requires “coverage for medical or drug treatments to correct or repair disturbances of body composition caused by HIV associated lipodystrophy syndrome including, but not limited to, reconstructive surgery, such as suction assisted lipectomy, other restorative procedures and dermal injections or fillers for reversal of facial lipoatrophy syndrome.” How do I access coverage?The provider who is undertaking the treatment may need to submit a request for prior authorization with your insurer. However, the law ensures coverage with a statement from a treating provider that “the treatment is necessary for correcting, repairing or ameliorating the effects of HIV associated lipodystrophy syndrome.” Please be sure that your doctor knows to include this important language in the request. What if I have applied for treatment in the past and been rejected?That does not matter. Your doctor can submit a new request for prior authorization and you will not be denied because you were rejected for the same procedure in the past. If you have further questions, contact GLAD’s legal information line at 617-426-1350, www.GLADAnswers.org, or AIDS Action Committee’s legal hotline at 617-450-1317.
HairToStay- Scalp Cooling Subsidy HairToStay is a nonprofit organization that offers need-based grants to offset the expense of scalp cooling systems for chemotherapy patients being treated in the United States. Subsidy recipients will usually be reimbursed up to $250 per month up to $750 total. About Scalp CoolingThere are two basic approaches to scalp cooling: Manual Scalp Cooling Systems and Automated Scalp Cooling Systems. Learn more about scalp cooling options. Scalp cooling purports to minimize chemotherapy induced hair loss by continuous application of precisely cooled caps to the scalp in stages before, during and after chemotherapy infusions. Scalp cooling systems are rented, not sold. Most insurance companies do not cover the costs of scalp cooling currently, but might if you ask for a cranial prosthesis. How to ApplyFirst, read the Eligibility Requirements below. If you qualify for a subsidy, download and fill out the Scalp Cooling Subsidy Program Application. (Aplicación en español) and submit it along with the documentation requested in the application. You can submit it by email HairToStay@pap-apps.org, by fax to 888-246-6527 or by US mail to HairToStay Subsidy Program, P.O. Box 219, Gloucester, MA 01930. Applications are accepted throughout the year. Eligibility Requirements
Notification and ReimbursementYou will usually be notified within one week of submission regarding the status of your application. If you have not heard back, please email us again. In order to be reimbursed, copies of statements from your scalp cooling treatment provider must be provided within one month of the invoice date. Additional Information and SupportIn addition to providing treatment subsidies, HairToStay is available to provide information to patients who are considering the use of scalp cooling, as well as guidance and support through the treatment process. If you have questions about scalp cooling in general, please email Patsy Graham at patsy@HairToStay.org. For all questions about the Scalp Cooling Subsidy Program please email HairToStay@pap-apps.org or call toll free at 800-270-1897. To apply: http://www.hairtostay.org/apply-for-a-subsidy/ -Thanks to Adi Chenki-Shapsa for sharing this resource.
SAGE Launches LGBT Age-Friendly Housing Website Home isn't just where we live - home is our safe place. That's why Services and Advocacy for GLBT Elders (SAGE) has created a first-of-its-kind housing website that empowers LGBT elders to find a welcoming place to call home. We know that housing discrimination is on the rise, and dependable resources are needed more than ever. Now, you can access housing policies and protections, and find out where LGBT age-friendly communities are being built via SAGE's new interactive map and resources. Editor’s note: current site content is limited, but this is a site worth watching and may be particularly useful to find resources outside of Massachusetts.
Welcome Family - Free Newborn Home Visit Welcome family offers a one-time nurse home visit to all mothers with newborns, regardless of age, income risk or other criteria. The visit is conducted by a nurse up to 8 weeks postpartum and lasts 90 minutes. The goal of Welcome Family is to serve as an entry point into the system of care for families in Massachusetts. Welcome Family is available to any mother with a newborn living in Boston and is also available in Springfield, Holyoke, Fall River, Lowell and Lawrence. During the visit the nurse assesses physical and emotional health and well-being, including breastfeeding, safe sleep, family planning, substance use, postpartum depression and interpersonal violence. The nurse provides education and referral to services as needed and addresses the mother’s specific questions or concerns. Please contact the Boston Public Health Commission, the agency managing the Welcome Family Boston program for more information, to request brochures and referral forms or to refer.
Welcome Family Boston Or for more information see the Welcome Family website. -Thanks to Marisa Iacomini and Andra Sobran for sharing this resource.
Yad Chessed – Emergency Assistance for Jewish Families Yad Chessed, which means “hand of loving kindness,” was founded in 1989 by Bob Housman to help Jewish families and individuals in need. Their programs support clients across Massachusetts by alleviating economic distress and providing ongoing support to help them reach financial stability. Programs Include:
-More Information: http://www.yadchessed.org/
MassHealth Managed Care Organization (MCO) Lock-In and Primary Care Clinician (PCC) New Referral Requirements Please see below for important MassHealth updates. MassHealth Plan Selection and Fixed Enrollment Periods & PCC Plan Referral Changes Starting October 1st, 2016, MassHealth will implement changes for members enrolled in either a MassHealth Managed Care Organization (MCO) or the Primary Care Clinician (PCC) Plan.
What is the new MassHealth Plan Selection Period?
Currently, MassHealth members who enroll in a Managed Care Organization (MCO) health plan may change plans at any time for any reason. Starting October 1st, 2016, MassHealth will implement a new 90-day Plan Selection Period for members enrolled in MCOs. Which means:
What are the MassHealth MCO health plans? The MassHealth MCO health plans are:
What health plans can a MassHealth member choose from during their Plan Selection Period? MassHealth members can choose from any of the MCO health plans listed above or the Primary Care Clinician (PCC) Plan. What is the Fixed Enrollment Period? The Fixed Enrollment Period will begin for members immediately following the 90-day Plan Selection Period end date.
Does this impact member’s ability to change their primary care physicians? No, members enrolled in an MCO can change to a different primary care physician in their MCO plan at any time. Do these changes apply to all members? No. These changes do not apply to the following individuals:
Changes to Primary Care Clinician Plan Referrals
Starting October 1, 2016, members in the Primary Care Clinician (PCC) Plan will need to get referrals from their PCC for the following services that did not previously need a referral:
For additional information, please see the presentation Changes to the MassHealth Managed Care Organization (MCO) and Primary Care Clinician (PCC) Plans available on the MTF (MA Health Care Training Forum) website. See a sample letter. -Thanks to Brooke Alexander, Senior Program Manager, Partners Public Payer Patient Access, for this article.
CMS Announces Notice for People with Marketplace Coverage and Medicare In June, the Centers for Medicare & Medicaid Services (CMS) announced an initiative to help people with Marketplace plans transition to Medicare after a call to action from more than 40 leading consumer advocates and health insurers- led by the Medicare Rights Center. The health insurance Marketplaces created by the Affordable Care Act (ACA) provide coverage options to people who would otherwise be uninsured. Many people currently in the Marketplace who will soon qualify for Medicare are unfamiliar with Medicare enrollment rules and timelines. A mismanaged transition to Medicare can result in higher health care costs, gaps in coverage, and even tax penalties- making adequate notice and supports critical to promoting the health and financial security of people new to Medicare. CMS recently released a new notice that people with Medicare and Marketplace coverage will receive. The notice informs these individuals that if they have Medicare, they are most likely no longer eligible to receive the premium tax credits to help pay for Marketplace plan premiums. The notice also provides useful information on how to ensure that you are enrolled in Medicare without penalties or gaps in coverage. Medicare Rights applauds CMS for providing enhanced notice and education to people with Marketplace plans who are also enrolled in Medicare. In addition, Medicare Rights supports ongoing efforts by the agency to reach individuals with Marketplace coverage who are approaching Medicare and will continue to work with CMS to ensure people appropriately transition from the Marketplace to Medicare. Advance notice and adequate education is fundamental to ensuring that people with Marketplace plans are prepared to enroll in Medicare. For more information on this notice and how CMS will target appropriate individuals, view their slide deck. -See the full Medicare Rights Center blog post. -Also see “Enrolling in Medicare when you have Other Types of Insurance” on MedicareInteractive.
Medicare Reminder – Medicare D Drug Coverage The amount you pay for your drugs through your Medicare private drug plan will probably change throughout the year. Your drug costs can change for various reasons.
How much your Medicare Part D plan pays and therefore how much you pay will change during the year. There are four different coverage periods for Medicare prescription drug coverage.
While nearly the full cost of brand name drugs counts towards reaching catastrophic coverage, your monthly premium and the 35 percent generic discount are not included in the $4,850 out-of-pocket costs needed to get out of the coverage gap into catastrophic coverage. When you reach catastrophic coverage you will pay either a 5 percent coinsurance on the cost of covered drugs or a copay of $2.95 for covered generic drugs and $7.40 for covered brand-name drugs, whichever is greater. -From Medicare Watch, The Medicare Rights Center, August 04, 2016.
Medicare Reminder – Part B Late Enrollment Penalties For each 12-month period you delay enrollment in Medicare Part B, you will have to pay a 10 percent Part B premium penalty, unless you have insurance from your or your spouse’s current job. -From Medicare Watch, The Medicare Rights Center, August 25, 2016.
Much Higher Premiums Tied to Plan Choices Even for the Very Poor Bad news from the state Health Connector at a recent board meeting. Since the Connector started offering coverage in 2006, its enrollees below the poverty level, like MassHealth enrollees, have been able to choose from any available managed care organization (MCO) with no premium charge. No more. People at all income levels will still have access to at least one "affordable" MCO - for people below 150% FPL, affordable means no member premium contribution - but other choices may mean substantially higher premiums. This will primarily affect the 43,000 people enrolled in Neighborhood Health Plan (24% of all ConnectorCare members) and the 5400 enrolled in Health New England. NHP is owned by Partners & the only plan to include the flagship Partners' hospitals and affiliated doctors in its network. HNE is owned by Baystate Health with 5 hospitals in Western Mass. NHP is the "affordable" plan only on the Islands and Baystate Health hospitals are in "affordable plans" only in the Franklin County region not in the rest of Western Mass. This means a person with little or no income now enrolled in NHP in Boston or HNE in Springfield for 2017 will either have to change plans (and probably change doctors) or go from no premium to $152 per month for one person or $304 per month for a couple. See ConnectorCare Contribution tables showing the monthly premium contributions for 2017 by Region and Plan Type.
Warning from IRS for those who got advance premium tax credits in 2015 but have not yet filed 2015 taxes: File or lose 2017 advance premium tax credits. In Massachusetts, that means ConnectorCare members in 2015 will lose ConnectorCare for 2017 unless they filed their federal taxes and "reconciled" the tax credit paid to their health plans to reduce premium charges for 2015. -From Health Announcement listserv, on behalf of Vicky Pulos, Mass Law Reform Institute, September 09, 2016. -See related Boston Globe coverage.
|