|
MGH Community News |
|
MGH Community News |
| November 2019 | Volume 23 • Issue 11 |
Highlights
Sections Social Service staff may direct resource questions to the Community Resource Center, Hannah Perry, 617-726-8182. Questions, comments about the newsletter? Contact Ellen Forman, 617-726-5807. |
New Social Security Representative Payee Portal The Social Security Administration has announce a new tool to make it easier for caregivers who serve as representative payees and oversee Social Security or Supplemental Security Income benefits for beneficiaries who are unable to manage their own benefits. The Representative Payee Portal provides a convenient way for individual representative payees with a my Social Security account to manage direct deposit, wage reporting, and annual reporting for their beneficiaries. You can learn more about becoming a representative payee and all the requirements by:
- From New Resource for Individuals Who Provide Care, Social Security Administration, November 14, 2019. |
| Feds Reduce Fuel Assistance to MA – Again
The federal Health and Human Services administration on Nov. 1 released $114.3 million in LIHEAP funds to Massachusetts. The state received $147.7 million in fiscal 2018, and $136.4 million in fiscal 2019. The federal government does not have an approved budget for fiscal 2020, which began Oct. 1. Therefore, it is working under a continuing resolution. Because of that, only about 90% of LIHEAP money has been released to states. If the House and Senate are able to reach a budget compromise, Massachusetts might receive a total allocation of about $127 million, said John A. Keeney, area program coordinator for New England Farm Workers’ Council Inc.. Statewide, more than 156,000 households received a benefit from the LIHEAP program last winter. |
Keeney, who serves on the National Energy and Utility Affordability Coalition’s public policy and advocacy committee, said the House wants to add $150 million to the LIHEAP budget to help low-income people pay for heat this winter. The Senate is looking at level-funding the national program. If the program is level-funded and Massachusetts receives 100% of what is earmarked to the state under a complicated funding formula, the commonwealth would still lose $9.5 million compared to last year. The state receives less in LIHEAP funds than it did 10 years ago. Keeney said Massachusetts has lost about $20.7 million, or 14.04%, of LIHEAP funding from fiscal 2018 to fiscal 2020. The only other states where the funding loss has been in the double digits are Connecticut (14.21%), and Rhode Island (10.9%). Across New England, New Hampshire has only lost about 1.6% in LIHEAP funding over the past two fiscal years, and Maine about .2%. Vermont’s funding has increased by 1.4%, Keeney said. Other states during the same period has seen significant increases in LIHEAP funding. For instance, Oklahoma’s share increased by 18.4%; Alabama, 16.1%; Louisiana, 15.1%; and Mississippi, 11.9%. Massachusetts received reduced allocations in fiscal 2018 and fiscal 2019 even though $250 million was added to the national LIHEAP budget in fiscal 2018, and an additional $50 million in fiscal 2019. What has rescued low-income households in Massachusetts is that the Legislature appropriated $30 million last fiscal year to supplement the LIHEAP program. Nineteen million dollars of that was used in fiscal 2019, and the remaining $11 million is allocated for this fiscal year. Keeney pointed out that currently the maximum delivered fuel benefit for someone at the federal poverty level is $1,140, and the maximum utility heating benefit at the federal poverty level is $905. Last year it was $1,660 and $1,150, respectively. There are different income guidelines and benefit levels. U.S. Rep. James McGovern, D-Worcester, in a phone interview, said the entire New England congressional delegation is working as a team to see if they can change what’s happening. McGovern said he believes the reason for Massachusetts getting less LIHEAP funding is because the funding formula that was changed by HHS a year ago is flawed. He said the new formula seems to favor Southern states that used electricity for both heating and cooling over Northern states. -See the full Worcester Telegram article.
Temporary Protected Status Extended for 7 Countries The U.S. Department of Homeland Security announced this month that recipients of Temporary Protected Status from six countries will be allowed to remain in the U.S. another year pending a federal class-action lawsuit. The extension benefits an estimated 12,000 immigrants who call Massachusetts home. DHS confirmed earlier that it would extend TPS designation for El Salvador due to the lawsuit. The move benefits an estimated 200,000 Salvadorans nationwide and 6,000 Salvadorans in Massachusetts. The second announcement expands the extension to include TPS holders from Haiti, Honduras, Nepal, Nicaragua and Sudan, until January 4, 2021. According to the USCIS website, the Temporary Protected Status (TPS) designation for Syria has been extended for 18 months through March 31, 2021. Those countries are at the center of class-action litigation challenging the Trump administration’s efforts to end protections for recipients who fled natural disasters, civil strife and other crises. More than 300,000 people in the U.S. have TPS from these countries, though the Trump administration has sought to end protections for them and order them to return to their native countries. An estimated 12,000 of these TPS holders call Massachusetts home, according to data provided by the Massachusetts Immigrant and Refugee Advocacy Coalition. Getting accurate estimates is more difficult, critics say, as some TPS holders may have self-deported under the Trump administration for fear of being detained and forcibly deported, advocates say. Critics of the program say TPS has become akin to amnesty for these immigrants, whose work permits are based on calamities more than a decade old. Immigrants and human rights advocates argue that their countries remain in dire straights, in part due to the original crises, and that they have built families and careers in the country they now call home. Some TPS holders have married U.S. spouses and become lawful permanent residents, but many argue they have sought to become green card holders but cannot because no path to citizenship exists for TPS recipients. They argue the Trump administration’s announcements to end TPS designation has thrown their lives into limbo, as their work permits are now valid for a few months instead of two years at a time. -See the full Mass Live article, with additional information from USCIS.
Court Blocks Trump Rule that Would Negatively Impact Patient Care This week, a federal court blocked a Trump administration rule that would have allowed health plans and providers to refuse to provide certain types of care they disagreed with on moral or religious grounds. Set to take effect on November 22, the rule would have permitted individuals to deny care even in circumstances where performing the refused service was a significant portion of their jobs, and even where the refusal could prevent patients from receiving the service altogether. The court found that this broad rule violated several statutes, including the Civil Rights Act of 1964 and the Emergency Medical Treatment and Labor Act that ensures access to emergency care. In addition, the court determined that the administration did not comply with proper rulemaking and used “factually untrue” arguments to justify this rulemaking. Proposed by HHS’ Office of Civil Rights more than a year ago, the rule was designed to protect ‘‘conscience rights’’ of health-care providers by boosting enforcement of at least two dozen laws already on the books that allow doctors, nurses, technicians, and other providers to opt out of procedures such as abortions or gender-change procedures to which they object. But many physician and health advocacy groups contended the rule would have disproportionately harmed certain groups of patients, including LGBTQ patients. Existing civil rights laws require careful balancing of the rights of providers and the rights of patients, and do not require employers to hire and employ individuals if accommodating those employees would create an undue hardship for the employer. For example, a surgical practice is not required to employ as a surgeon a doctor who is morally opposed to surgery. This rule would have upended such balancing by requiring employers to staff around objecting health care providers. The court found that the rule could force employers to double or even triple staff under some circumstances, driving up costs in the health care system and reducing the ability of employers to adjust staffing appropriately. In addition, the rule failed to establish exceptions for emergency situations, potentially putting the lives and health of patients at risk. The administration claimed this rule was necessary because of a large spike in complaints from health care workers about perceived violations of their religious and conscience rights, announcing they had received 343 such complaints in 2018 alone. But during oral arguments, the administration admitted that they had not actually received such a huge influx of complaints and the true number was around 20. ‘‘We are heartened by today’s ruling, and we will not stop fighting to prioritize patients’ need for standard medical care over health-care personnels’ personal religious or moral beliefs,’’ the National Family Planning and Reproductive Health Association said in a statement. The rule was part of the administration’s broader efforts to bolster the rights of religious health providers and restrict abortion access. The administration prevailed in earlier lawsuits against a rule that barred federal family planning grants from going to providers that perform abortions, most notably Planned Parenthood, and has also cut international aid to groups that provide or offer abortions. Read more about this court’s decision. Read Medicare Rights’ comments on the proposed rule. - See the Medicare Rights Center blog post and the full Boston Globe article.
Mass. RMV is Now Offering Non-Binary Gender X Licenses and ID Cards The Massachusetts Registry of Motor Vehicles announced this month that as part of its system upgrade, it is now allowing residents to choose a gender designation of X on their driver's licenses or state ID cards. The registry said it will now recognize three gender designations: male, female and non-binary. Massachusetts joins several other states that have legalized gender-neutral license designations, including California, Maine and Idaho. The agency's move circumvents the Legislature, which has been unable to complete work on a bill for several years. Senate President Karen Spilka, an Ashland Democrat, has tried to pass legislation to make a "gender X" designation available on state licenses and other identification documents, but each time it passed the Senate it stalled out in the House. The bill that cleared the Senate also would allow residents to amend their birth certificates to reflect the non-binary gender X. - See the full WBUR story.
Kuehn Foundation Heading Effort to Create Affordable-Housing-Search Site The Kuehn Charitable Foundation and several state housing agencies and affordable housing advocates are working on what will be Massachusetts’ biggest searchable database of deed-restricted affordable housing. Dubbed The Housing Navigator, it aims to be a one-stop online shop for all affordable housing in the state, easing an often-tedious search for subsidized apartments. Kuehn and Citizens Housing and Planning Association — a housing advocacy group — are partnering with state agencies that finance affordable housing in Massachusetts to create a comprehensive, searchable database of what are probably hundreds of thousands of income-restricted, rent-subsidized apartments across the state. They’re gathering data and starting to test the website with potential users — both tenants and the housing advocates who work with them — with a goal of launching it sometime next year. The system will be a major upgrade from the 20-year-old Mass Access Registry, which covers some, but far from all, affordable housing in the state, said Rachel Heller, chief executive of the citizens housing association. And it’ll be broader than a database maintained by the City of Boston (MetroList). The groups are aiming to make the Housing Navigator as user-friendly as possible for would-be renters to search and for property managers to post listings. The idea is to cover units funded under a wide range of federal, state, and local programs — all in one place. The Housing Navigator will be one of the firsts of its kind. Minnesota is the only other state in the nation that offers a one-stop online tool collecting all available affordable housing listings, officials said. Massachusetts lacks 186,775 units needed for households earning less than 50 percent of their area’s median income, according to a 2016 report from the National Low Income Housing Coalition. The situation is dire for the state’s most needy residents. Massachusetts has fewer than half as many affordable units of housing available as it needs to serve extremely low-income residents — defined as households earning 30 percent or less of their area’s median income, according to an April report from the Federal Reserve Bank of Boston. When people are housing-burdened, a federal definition meaning they spend more than 30% of their income on housing costs, it often means they must forgo spending on health care, food, childcare, or other necessities. A single financial shock can cause this group to fall behind on rent, leading to eviction or even homelessness, according to the report. In a state with a wide array of affordable housing programs, and where cities such as Boston and Cambridge have long required new buildings to set aside units for lower-wage tenants, a surprising number of low-cost apartments can fall under the radar. Municipal boundaries also come into play. While some communities have programs that are relatively easy to search, they’re often run at the local level. Looking for housing in other cities and towns can mean starting anew — a time-consuming and complicated process — and that limits people, Gilbert said. Eventually, Jennifer Gilbert, the executive director of Kuehn said, they hope to upgrade the site to make it easier for people to not just find potential apartments but to apply to rent them. It’s the sort of thing that’s common in the world of market-rate rentals — where you can rent an apartment online without ever seeing it in person — but a rarity when it comes to affordable housing. That, Gilbert said, needs to change. Learn details about plans for The Housing Navigator via an archived webinar. Highlights of planned features include:
Limitations
-See the full Boston Globe article, the Boston Herald article, and the webinar.
Ride United – United Way Offers Free Lyft Rides United Way Worldwide recently announced the launch of Ride United, a transportation access initiative that will help those in need overcome transportation barriers. Ride United launches with initial support from General Motors and Lyft, and leverages the strengths of local United Ways and the 211 network to address unmet transportation needs for individuals and families. The first cities involved in this initiative are partnering with Lyft to provide free rides to eligible 211 clients in need of transportation for employment, health, and other needs. In the U.S., 45% of people don’t have access to public transportation, and roughly 10.5 million people don’t have access to a vehicle. 211s in more than twenty-five local markets, including Boston, will be able to schedule Lyft rides for eligible clients without other transportation options. “Every year, the 211 network receives more than 230,000 transportation requests, and on average 25% of these can’t be met with existing resources,” explained Rachel Krausman, Senior Director, 211, United Way Worldwide. “In 2018, we partnered with Lyft in 12 cities and provided 12,000 free rides for employment, medical care, and veterans’ services to help fill this gap and saw how transformational a single ride could be. Through Ride United, more United Ways and 211s will work with their communities to close transportation gaps throughout the country.” Details Ride United is a pilot program approved at least until June 2020. Ride United generally offers a one-time ride, but depending on budget and need, they may be able to extend it, such as for someone whose MBTA The RIDE approval is pending. The program is operating within the Boston and Springfield areas. Covered communities near Boston: Boston, Brookline, Charlestown, Chelsea Cambridge, Everett, Malden, Medford Somerville, Roslindale to Boston. Ride United MAY be able to offer local rides within Quincy or Quincy to Brockton as funding allows, but probably not, as an example, Quincy to Boston during rush hour.) At the end of a month if money is left in budget they may be able to be more flexible and offer longer trips. In this area there are three acceptable uses:
How It Works The client calls 211and they assess for transportation options. There is no income limit. If the client is eligible for the program, 211 will schedule and pay for the round-trip Lyft ride. 211 staff will tell client what vehicle looks like and where to meet it. The client does not need to have a cell phone. - Source: https://www.unitedway.org/the-latest/press/united-way-launches-ride-united with additional information from the 211 call center. -Thanks to Kristen Risley for sharing this resource.
Massasoit to Offer Tuition-Free College for Low-Income Boston Students Massasoit Community College is the fifth community college in Massachusetts to join Boston’s Tuition-Free Community College Plan, which funds up to three years of community college for eligible low-income Boston students. The plan was launched in April 2016 in an effort to make higher education accessible to those who may not be able to afford it. Program participants will be able to attend courses at Massasoit’s three campuses in Middleboro, Brockton and Canton. The addition of Massasoit to the program makes new associate degree programs available to participating students, including: diesel technology; heating, ventilation and air conditioning (HVAC); veterinary technology; and architectural technology. Massasoit Community College joins other participating colleges: Bunker Hill Community College, MassBay Community College, Roxbury Community College and the Benjamin Franklin Institute of Technology. To be eligible to participate, students must: be a Boston resident; receive their high school credential within 12 months of starting the program; be eligible for a Pell Grant as determined by the U.S. Dept. of Education; require no more than three developmental courses by the start of the semester; and have low to moderate household income per Housing and Urban Development guidelines. For students who do not receive full Pell coverage, the plan covers remaining tuition and mandatory fees for up to three years of community college. For students whose tuition and fees are fully covered by a Pell grant, the plan provides up to $1,000 for college-related expenses, such as books or transportation, according to plan guidelines. Tuition-Free Community College Plan participants can also extend their education to a four-year state university or University of Massachusetts campus through Boston Bridge, a program that allows participants to complete their bachelor’s degree without tuition fees or other mandatory fees. - See the full Enterprise article.
Upcoming Medicare Coverage Improvements for Treatment for Opioid Use Disorder The Centers for Medicare & Medicaid Services (CMS) recently finalized a rule that expands Medicare coverage for Opioid Use Disorder (OUD). Recent legislation, the Substance Use Disorder Prevention that Promotes Opioid Recovery and Treatment for Patients and Communities (SUPPORT) Act, established a pathway for this more comprehensive Medicare coverage of OUD services. Beginning on January 1, 2020, Medicare Part B will cover OUD treatment—including methadone for Medication Assisted Therapy (MAT)—furnished by an Opioid Treatment Program (OTP) under a bundled payment mechanism. This means a significant improvement in access to OUD care for people with Medicare, including for those who are dually eligible for Medicaid. Allowing Medicare Part B to pay for methadone as part of a MAT program is a welcome reform. Historically, methadone has only been covered by Medicare for outpatient pain management, not for opioid addiction, despite its effectiveness in treating OUD being well-documented. Specifically, it has not been reimbursable by Medicare Part B because under statute, it can only be dispensed and administered by an OTP for MAT, and OTPs have been ineligible for Medicare participation. The SUPPORT Act and this final rule from CMS eliminates this coverage gap. Starting in 2020, OTPs will be permitted to enroll as Medicare providers, and OTP services under the payment bundle will be available without cost-sharing for Medicare beneficiaries. These services include:
In addition to the OTP provisions, the final rule establishes a separate bundled payment system for OUD treatment services furnished in an office setting. Unlike OTP services, services provided in an office setting will not have cost-sharing set at zero, but we hope that CMS will consider creating new pathways in the future that eliminate cost barriers for OUD care. To further improve access to OUD treatment, both OTPs and providers in office settings will be permitted to furnish substance use counseling, individual therapy, and group therapy through telehealth technology, extending the reach of these important services. Historically, services that are covered by both Medicare and Medicaid may lead to confusion and difficulty accessing care for beneficiaries. This rule creates more overlap between the programs for OUD care and could result in access issues as beneficiaries transition from Medicaid to Medicare coverage for OTP services. In the final rule, CMS pledges to provide guidance, education, and outreach for transition issues and directs both OTPs and state Medicaid officers to ensure that people who are dually eligible for both Medicare and Medicaid do not face any issues accessing OUD care through Medicare. - See the full Medicare Rights Center blog post.
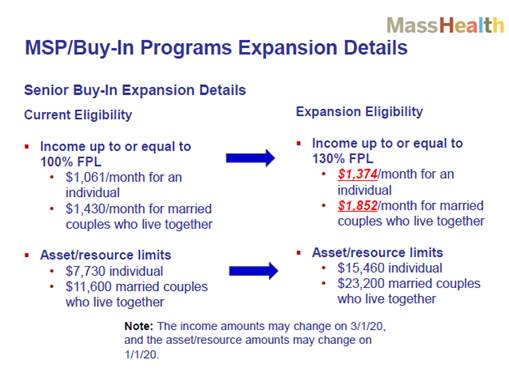
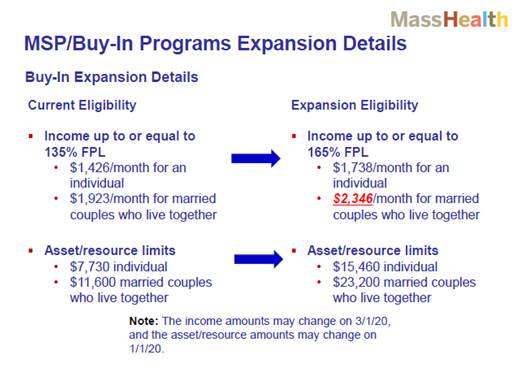
Medicare Savings Plans – Buy-In Program Eligibility Expansion Background Medicare Savings Programs (also known as the "MassHealth Buy-in" Programs) help older residents and people living with disabilities save money on their Medicare coverage. Low income beneficiaries may qualify for Medicaid (MassHealth) assistance for Medicare premiums and cost-sharing. Buy-In Under the standard Buy-In MassHealth pays for Medicare Part B premium. It also conveys automatic eligibility for the Medicare Part D Extra Help. Senior Buy-In Under Senior Buy-In:
MSP/Buy-In Programs Eligibility Expansion The State Fiscal Year 2020 budget included language expanding eligibility for the MSP/Buy-In programs; it increases the income and asset/resource limits for these programs. It is estimated that about 25,000 Massachusetts residents with Medicare will be newly eligible for these programs under the expansion. Approximately 15,000 Buy-In members would become eligible for Senior Buy-In under the expansion. MSP/Buy-In Programs Expansion Details
MSP/Buy-In Programs Effective Dates (under SSA rules) Effective Dates
MSP/Buy-In Programs Application Process Applications submitted before January 1, 2020 will use the current income and assets/resource limits. MassHealth is working on a process to re-determine all members currently on Buy-In, using the new income limits to see if they would become eligible for Senior Buy-In. Until this process is in place beginning January 1, Buy-In members can contact MassHealth Customer Service at: (800) 841-2900 (TTY: (800) 497-4648), to check if their benefits can be redetermined using the new rules. MassHealth is expanding the Buy-In Programs in two phases:
-See the full Mass Health Training Forum training slides.
MassHealth Has Eliminated Co-Pays on Smoking Cessation Products Effective September 25, 2019 MassHealth has eliminated co-payments on products that help people quit smoking, including nicotine replacement therapies (NRT), like gum, patches, and lozenges. What Should Members Know?
For information about quitting smoking or vaping go to www.mass.gov/service-details/quit-nicotinetobacco-or-support-someone-in-their-quit-attempt or visit the Helpline at MakeSmokingHistory.org -See the full MassHealth Training Forum webinar slides.
Medicare Advantage Plans May Offer Additional Supplemental Benefits in 2020 for Those with Chronic Illnesses Medicare Advantage Plans can offer Supplemental Benefits not covered by Original Medicare. These items or services do not need to be provided by Medicare providers or at Medicare-certified facilities. Instead, to receive these items or services, you need to follow your plan’s rules. Some commonly offered supplemental benefits are:
For the most part, supplemental benefits must be primarily health-related. Beginning in 2020, however, Medicare Advantage Plans can begin covering supplemental benefits that are NOT primarily health-related for beneficiaries who have chronic illnesses. These benefits can address social determinants of health for people with chronic disease. A social determinant of health is a part of your life that can affect your health in some way, such as not having access to transportation. Examples of the kind of benefits that plans can now cover are:
In order to be eligible for this new category of supplemental benefits, you must be considered chronically ill. This means that you:
If you meet the above criteria, a Medicare Advantage Plan may offer you one of these new benefits if it has a reasonable expectation of improving or maintaining your health or function. Since Medicare Advantage Plans will be able to create sets of supplemental benefits for people with specific chronic illnesses, not every member of a Medicare Advantage Plan will have access to the same set of benefits. For example, a plan might cover services like home air cleaning and carpet shampooing to its members who have asthma. A member of that plan who has asthma may be able to get these services covered, while a member who does not have asthma may not. Before enrolling in a Medicare Advantage Plan that has these new supplemental benefits, check if you meet the plan’s criteria for coverage. Contact your plan to find out how to access these and other supplemental benefits. - From What are supplemental benefit (sic)? Dear Marci, Medicare Rights Center, Tuesday, November 12, 2019.
Medicare Reminder: Patient Advocacy - Filing a Quality of Care Complaint If you have a concern about the quality of care you receive from a Medicare provider, your concern can be handled by the Beneficiary and Family Centered Care-Quality Improvement Organization (BFCC-QIO) for your area. The BFCC-QIOs are made up of practicing doctors and other health care experts. Their role is to monitor and improve the care given to Medicare enrollees. BFCC-QIOs review complaints about the quality of care provided by:
Examples of situations that you might wish to file a quality of care complaint about include:
Two ways that the BFCC-QIO might review this complaint are:
Livanta and KEPRO are currently the two BFCC-QIOs that serve the entire country. KEPRO services Massachusetts: KEPRO
Legislation Seeks to Protect Tenants from Unfair Stigma & Permanent Eviction Records Having an eviction record is creating a devastating barrier for tenants looking for housing. A tenant was rejected for over 100 apartments and was homeless for a year because of one eviction case that her landlord filed because he wanted to sell the building. She did nothing wrong. She moved out and her case was dismissed. As soon as an eviction case is filed a tenant has an eviction record. Regardless whether they did anything wrong or were actually evicted, the mere fact that they were party to an eviction or housing case is being unfairly held against tenants when they try to rent a new place. State legislation “An Act promoting housing opportunity and mobility through eviction sealing (HOMES)” seeks to protect tenants and improve their chances of finding new housing. PasstheHomesAct.org, in collaboration with Mass Law Reform Institute, has created a fact sheet, excerpted below: Eviction records are publicly available forever regardless of the outcome The outcome of a case should matter Vulnerable people are at risk of eviction Children are listed on eviction complaints
For More Information visit www.passthehomesact.org or:
Trump Administration’s Third Different Attack on SNAP For the 3rd time this year, the Trump Administration is trying to take Supplemental Nutrition Assistance Program (SNAP) off the tables of very low-income households. The proposed rule, which is currently open for public comment, would standardize and cap Standard Utility Allowance (SUA) calculations nationwide rather than allow states to continue to adjust the SUA to accommodate for differences in utility costs and rates. Under current federal SNAP rules, states have the flexibility to set SUA amounts that are used to calculate shelter costs for low income households. States historically have set their utility allowances to cover most SNAP household energy expenses during the highest energy usage months in the state or region. This SUA option simplifies the SNAP math and streamlines the state process for determining benefits. USDA has proposed a ”one-size-fits-all” rule that would force many states lower the value of allowed utility expenses to a limit set by USDA. Such a sweeping change would gravely affect high energy cost states like MA, where costs of energy and shelter (rent or home ownership) are some of the highest in the nation.
Which Massachusetts Households will lose SNAP benefits? Examples of the harm:
Public Comment -See the full fact sheet. Additional material from SNAP Cuts, Medicare Premiums, Medicaid Waivers, Justice in Aging, November 15, 2019 and Trump Administration attacking SNAP, again - MLRI call on MA harm on 11/12, November 04, 2019.
Industry Group Says 1 In 4 Nursing Homes at Risk of Closing One quarter of the nursing homes in Massachusetts are at risk of closing, according to an industry trade group. The Massachusetts Senior Care Association reported this month that an analysis conducted by the firm CLA and presented at the group's annual meeting concluded that 95 nursing homes are in danger of closing across the state. The report underscores the need for "immediate action" to prevent the displacement of thousands of frail elder and disabled residents, and the loss of jobs held by thousands of people who work at the homes. Homes are at risk due to underfunding from the state, rising labor costs, and competition from assisted living and home care operators, the association said. The Legislature boosted funding for nursing homes in this year's budget and created a Nursing Facility Task Force, which is scheduled to meet in Boston on Friday, Nov. 22 at 2:30 p.m. "Our report shows that many Massachusetts nursing facilities have been operating at negative margins for the past five-plus years, which simply is unsustainable," Michael Slavik, of CLA, said in a statement released by the association. - See the full WBUR story.
The SSI Restoration Act of 2019 This legislation would modernize SSI rules and requirements that haven’t been changed for decades. In addition to raising the $2,000 resource limit, for example, the Act would increase the amount of income a person could keep from sources like Social Security. Currently, people receiving SSI are not allowed to keep more than $20 of income they receive from Social Security. This means older adults receiving SSI and Social Security (over half of all older SSI recipients) would be able to use more of their limited Social Security income to supplement their SSI benefit. The bill would also make improvements, such as removing a marriage penalty, so that couples could receive their full SSI benefit rather than a reduced amount. The bill would also eliminate benefit reductions that occur when people are able to live with others to save money. In a statement, Justice in Aging said “Improvements such as these are important to fulfilling SSI’s goal of helping those most in need who would not otherwise have enough income to get by. We support this legislation because it will ensure that, rather than keeping people out of the program because of outdated restrictions, we will be able to provide support to those who need it.” Most of the SSI eligibility rules have not been updated since the program was signed into law by President Nixon over 40 years ago. The economy has changed since then and some of the rules of the program can make people’s financial problems even worse. For example, the amount of income a beneficiary is allowed to receive from other sources (such as a pension) without having their benefits reduced is $20. The cost of living today is more than 5.5 times what it was in 1972, meaning $20 today is equivalent in purchasing power to about $3 in 1972 dollars. In addition, the asset limit for the program–$2,000–has not been updated since 1989. Under the Act, several needed updates to the program’s eligibility rules would be made.
- See the full Justice in Aging Policy Issue Brief.
Former Hyde Park Middle School to Become New England’s First LGBTQ-Friendly Senior Housing Boston city officials this month designated a developer to turn a former Hyde Park middle school into the first LGBTQ-friendly senior housing complex in New England. The unanimous vote by the city’s Public Facilities Commission was a victory for members of the city’s LGBTQ community, who have been pushing for such a project for more than five years. The state’s LGBT Aging Commission estimates that 65,000 older LGBTQ adults live in Massachusetts, many of whom can’t depend on family members as caregivers. While the new apartments will be open to all residents over 62, there will be special “cultural competency” training for staff and residents to assure that LGBTQ seniors can feel comfortable there. “There’s a pent-up demand for senior housing that’s affordable but also safe and welcoming for LGBT seniors,” said Aileen Montour, president of LGBTQ Senior Housing Inc., a nonprofit that will be a co-owner and work in partnership with the developer on programs and services for the development. “This is a first for Boston, for Massachusetts, and for New England.” The plan will create 74 affordable and market-rate apartments that will be ready in the next few years. Of the 74 total income-restricted rental units in the new Barton Rogers development, eight will be rented to households of individuals who are homeless or who require rental assistance. Another eight will be deeply affordable units for seniors whose income is between approximately $25,000-$40,000 per year. In addition, 34 units will be available to households earning less than 60% AMI (about $55,000 for a two-person household). The remaining units will be rented to households earning up to 80% AMI (8 units) and 100% AMI (16 units).Bob Linscott, a board member of the nonprofit and assistant director of the LGBT Aging Project at Fenway Health, said the hope is to forge a culture that can serve as a model for tolerance and acceptance at other senior housing in the region. “The No. 1 issue for LGBT seniors is housing,” Linscott said. “There’s a huge panic about where we’re going to go when we can’t take care of ourselves. There’s a big fear of going to a place where people will be bullied and harassed by the same people who bullied and harassed them decades ago.” Adaptive reuse of the Rogers School is part of a larger campaign in Boston to make former schools and other public facilities available for housing and community gardens, said Sheila Dillon, the city’s chief of housing and director of neighborhood development. Over the past five years, the city has turned over 3 million square feet of surplus property, she said. There are about 30 senior housing complexes that are open or being planned nationally that are designated as LGBTQ-friendly. Pennrose is currently operating one, John C. Anderson Apartments in Philadelphia, and is in the process of developing another, Haven Green in New York’s Little Italy. Under federal anti-discrimination law, developers can’t set aside units for gay and lesbian seniors, but such developments are typically marketed to LGBTQ seniors. “We feel like we know how to do it,” said Charlie Adams, the Boston-based regional vice president of Pennrose, which develops and manages multifamily housing in 15 states and the District of Columbia. “We feel like we’re sensitive to some of the issues. A lot of times people feel, when they move into senior housing, that they have to go back into the closet. We want to have a place where they don’t have to do that.” - See the full Boston Globe article and additional material from Universal Hub.
Mass. Has the First Jail in The Country That's Also a Licensed Methadone Treatment Provider The Franklin County Jail is thought to be the first jail in the country to become a licensed methadone treatment provider. Franklin County is among seven jails in the state that will receive about a half million dollars each to participate in a new pilot program to provide all three addiction medications. Not only does that mean that half of the state jails are doing this, but they all are now also licensed by the state Department of Public Health. DPH will collect data on outcomes in the hopes of reversing the grim statistic that the opioid overdose death rate in Massachusetts is 120 times higher for those recently released from incarceration, compared with the rest of the adult population. Three years ago the Franklin County Jail, in Greenfield, became the first in the state to offer buprenorphine, largely because of Sheriff Christopher Donelan. "We don't judge and we don't punish; the judge punishes," Donelan says. "Our job is to treat people with dignity and respect and to keep people safe and to do our best to make them better because no one is serving a life sentence here, so they're all coming back to our communities." Donelan says his approach has reduced recidivism. He thinks all jails should focus on treatment. "I was determined when I became sheriff that this was going to be a locked treatment facility," he says. "If somebody is sick, we take care of them. If they're sick with kidney or heart disease, we give them the treatment and medication. If they're sick with addiction, we should give them the treatment and medication for that." Recently Donelan accomplished another first: Rather than hire an outside provider, his jail is now the only one in the country licensed to provide methadone itself. By law, methadone must be distributed by a federally licensed facility and comply with myriad regulations. Each person coming in to the jail is screened for drug use and withdrawal symptoms. They're asked if they've been prescribed medication and if they want it. About half say they're addicted to heroin. Correction officer Lee Terrell says providing medications has helped the jail. "I think it's working," he says. "I think violence in the facility has gone down. We used to get a lot through the mail; there used to be a lot of contraband. That has come to minimal, if anything." Many correction officials have refused to provide all three addiction medications that are available. Officials have been more open to providing naltrexone, which goes by the brand name Vivitrol and typically is given right before someone is released to block the effects of opioids. The other two medications, buprenorphine or methadone, are opioids, and many correction officials say those medications are too easily diverted for illicit use. But Ramirez says that's not true. "The process we do here, it's almost impossible," he says. "There's no way. I mean if you attempt it you're just dumb."
Those held in Massachusetts jails or houses of correction are either awaiting sentencing or serving sentences of up to two-and-a-half years. Those with longer sentences go to prisons run by the Department of Correction. The same law that established the jail pilot program also required four of the 16 DOC-run facilities to provide all three addiction medications. The DOC has not yet contracted with a methadone provider. "If the goal is to not die, this is effective," Schwartz says. "But if the goal is to not return to jail and live a life of meaning and purpose, now we're talking about something different, and a pill is not going to help that. It may be part of the picture but it has to be a larger constellation. " State health officials hope to outcome data from the pilot program in two years. - See the full WBUR story.
Many Colleges Still in Denial About Need for Recovery Services Despite the concentration of colleges in the region, and the heightened attention to opioid addiction in Massachusetts, few resources are available on campuses to serve young adults struggling with substance use. “Most of the Boston schools are still kind of in the early stages” of addressing addiction, said Timothy Rabolt, executive director of the Association of Recovery in Higher Education, a national group of collegiate recovery programs and advocates. “It’s turning in the right direction. It’s just not quick enough.” Many colleges around the country aren’t aware of the need, or just don’t want to acknowledge it, Rabolt said: “The overall feeling from the top administrators is ‘We don’t have those students at this school.’ ” Of course, all colleges have such students. With drug and alcohol use rampant on campuses, some students inevitably run into difficulties, while others are recovering from addiction and need help staying sober in what has been called a “recovery-hostile environment.” But tackling drug use on campus means acknowledging it, and that can be a sensitive issue. Indeed, two of the several institutions contacted by the Globe for this article — the Massachusetts Institute of Technology and Boston College — declined to even discuss what services they provide for students in recovery or struggling with substance use. And yet, as Rabolt puts it, “This is something where students’ lives are on the line.” The college years are a crucial interval in a person’s life, an age when newfound freedom combined with stress and campus culture can lead many to hazardous behaviors. “This is the highest-risk period for the onset of substance use disorder,” said John F. Kelly, director of Massachusetts General Hospital’s Addiction Recovery Management Service, a program for teenagers and young adults. Collegiate recovery programs, usually sponsored by university health or counseling services, can attract young people in recovery who wouldn’t otherwise attend college, Kelly said. In addition, he said, the “substance-free” activities that such programs sponsor may even have a ripple effect on college culture and prevent some students from falling into unhealthy drug use. Whether or not opioids are prevalent on campus, Rabolt said, the opioid crisis has played an important role, by making addiction, at last, a topic of conversation. About 200 colleges nationwide have some type of program for addiction and recovery, Rabolt said. The best ones have at least one full-time staff member and a space for people to meet. - See the full Boston Globe article.
Some Boston Neighborhoods Face Severe Child Care Shortage and it’s Unaffordable Almost Everywhere The chasm between supply and potential demand for child care is so wide across much of Boston that in some neighborhoods, there aren’t enough seats for roughly half the children, according to a new report from the Boston Opportunity Agenda. Only about one in four children under the age of 5 has access to high-quality programs, as defined under state and national standards, the report found. That shortage is most pronounced in Roslindale, West Roxbury, and Hyde Park, which lack high-quality slots for nine out of every 10 children, the report found. The report from the Boston Opportunity Agenda, a public/private partnership focused on education, provides what child care advocates say is the first detailed picture of some of the most vexing challenges in the city’s early education and care programs. One of the biggest problems Boston has tried to solve is, how many children are we trying to serve? In some communities, they don’t even know, and are blaming each other” for gaps and surpluses, said Amy O’Leary, a director at Strategies for Children, a Massachusetts organization that advocates for high-quality early education programs. The report found child-care shortages are most acute for children aged 2 and younger, with the biggest squeeze in East Boston, where there are only enough slots for 1 in 10 infants. The richest supply, researchers said, is in the Back Bay and Beacon Hill, where the gap is less than half that size. Early education programs are somewhat easier to find for children between 3 and 5 years old because of preschool and public kindergarten easing the care crunch. But one problem is inescapable: the high cost of care. Federal guidelines define affordable care as care that costs no more than 10 percent of a family’s income. By that standard, the average cost of infant care is unaffordable for all neighborhoods in Boston, the report said. The percentage of income spent on child care in the Back Bay and Beacon Hill is just over 10 percent, compared with over 55 percent of the median family income in Roxbury and nearly 40 percent in East Boston. “Child care in Boston affects everyone, no matter where you live, no matter your income bracket, no matter what you look like. It is not affordable for anybody, and it’s difficult to access,” said Kristin McSwain, executive director of the Boston Opportunity Agenda. A recent survey by the City of Boston found that more than one-quarter of stay-at-home parents, the vast majority of them women, couldn’t work because they lacked day care. Nearly 60 percent of those parents cited cost as the biggest obstacle, and also found that parents of children under 2 had the hardest time finding available slots. The challenges facing child-care providers are also daunting. They say they struggle to keep quality workers and provide decent wages, without making the cost of care unaffordable for families. The report made several recommendations, including a call to create stronger partnerships among providers, the city, and various agencies and nonprofits. Those partnerships would be able to collect more detailed data that could more finely pinpoint actual demand by neighborhoods. It also suggested businesses work more closely with providers to subsidize some slots for employees’ children. This, the report said, could create consistent care options for workers, while also providing steadier revenue for child-care facilities. - See the full Boston Globe article.
Judge Blocks Trump’s Plan to Bar Immigrants Who Can’t Pay for Health Care A federal judge this month blocked the Trump administration from implementing a policy, reported last month (Trump Administration’s Plan to Require Immigrants Show Health Insurance, MGH Community News, October 2019) that would require immigrants to prove they have insurance or the financial resources for medical costs in order to obtain a visa. The ruling, by Judge Michael Simon of the Federal District Court in Portland, Ore., was the latest in a string of court decisions to derail administration initiatives that would limit the admission of certain legal immigrants into the United States. Judge Simon issued a nationwide temporary restraining order preventing the government from carrying out a proclamation by President Trump that would have gone into effect on November 3rd. Mr. Trump’s Oct. 4 proclamation ordered consular officers to bar immigrants who could not prove they had health insurance or the ability to pay for medical costs once they become permanent residents of the United States. The president had justified the policy on the grounds that immigrants were more likely to be uninsured, and that “costs associated with this care are passed on to the American people in the form of higher taxes, higher premiums, and higher fees for medical services,” the measure said. Legal immigrants are three times as likely as American citizens to be uninsured, according to a Kaiser Family Foundation study. Lawyers from Justice Action Center, Innovation Law Lab and the American Immigration Lawyers Association argued that the policy was “plainly illegal” and that it would cause immediate and irreparable harm.
“This new requirement rewrites our immigration and health care laws,” the lawyers wrote in a motion seeking a temporary restraining order. They noted that the policy could effectively bar up to 375,000 “otherwise qualified immigrants each year.”
- See the full New York Times article.
Elder Economic Insecurity High in MA Even in a strong national economy, half of older Americans living alone and nearly one-quarter of older couples struggle to afford basic necessities, according to a report that lists Massachusetts as a leading state for “elder economic insecurity.” Massachusetts tops all states in the share of single people over 65 whose income doesn’t cover living expenses such as food, housing, health care, and transportation. More than six in10 here fall short, according to the elder economic security standard index released Tuesday by the Gerontology Institute at the University of Massachusetts Boston. The state ranks third, after Vermont and New York, in economic insecurity for seniors in two-person households. Nearly 30 percent in Massachusetts fall below the index. “It really comes down to the cost of living, particularly the cost of housing and health care,” said UMass Boston gerontology professor Jan Mutchler, director of the institute’s Center for Social and Demographic Research on Aging, which has tracked data on income and living costs for older adults over the past decade. “Some of the same things that make Massachusetts a good place for younger people to get jobs are also driving up the cost of housing for seniors.” About 300,000 seniors in Massachusetts are considered economically insecure — and about 10 million seniors across the country, according to the UMass Boston index. The cost of living for older adults in Massachusetts ranges from $26,220 to $39,408 a year for a single person and from $38,424 to $51,612 for a couple, depending on whether they rent, own a house that’s been paid off, or own a house on which they’re paying a mortgage, the index calculates. In Massachusetts, a hub for higher education and well-paying industries, the findings from the report belie the popular image of prosperous retirees with disposable income. Researchers found many seniors fall into an “economic security gap” where their incomes — which include Social Security and, for some, wages, savings, and pensions — are too high to qualify for public benefits but too low to achieve economic stability. Those who can’t get family help sometimes resort to skimping on food or medicine, Mutchler said. “We hear a lot about people making all kinds of adjustments,” she said. “They can’t avoid paying their rent, but they keep their heat down in the winter or don’t turn on their air conditioning in the summer. Some of them don’t eat as well as they should, or don’t take the medication they need, or don’t go to the doctor when they should.” The high levels of senior economic insecurity documented in the UMass Boston report should spur policy makers to find ways to create more affordable housing, help older adults pay for rising medical costs, and provide relief from soaring property taxes, said Villers. Carolyn Villers, executive director of the Massachusetts Senior Action Council, a statewide advocacy group based in Quincy, said the waiting list for affordable senior apartments is seven or eight years in some Massachusetts cities and towns, while some seniors spend 20 to 30 percent of their monthly income on health insurance premiums. The report recommended, among other things, efforts to protect Social Security benefits, which account for at least 90 percent of the income for more than half the older adults who can’t afford essential living expenses. It also proposed keeping older employees in the labor force longer at a time when many businesses and other organizations are finding it difficult to attract workers. “A lot of [baby] boomers are crossing that retirement threshold and aren’t really prepared for the costs they’re going to face,” Mutchler said. -See the full Boston Globe article.
America's 'Shame': Medicaid Funding Slashed in U.S. Territories Right now, there are dozens of patients — U.S. citizens — in New Zealand hospitals who are fighting the clock. They have only a few weeks to recover and get home to the tiny island of American Samoa, a U.S. territory in the South Pacific. "We have a cancer patient that is coming back in December," says Sandra King Young, who runs the Medicaid program in American Samoa. "We can only give him six weeks of chemo, radiation and surgery. He has a good chance of survival if he has the full year of treatment, but not six weeks. The patient and family understand, and since they have no money, they have agreed to come back." The federal money to fully fund the Medicaid program in American Samoa and in all other U.S. territories is about to run out. As a consequence, the off-island referral program to treat conditions that the territory doesn't have the local capacity or facilities to treat — the program that brought these patients to New Zealand — is getting shut down. "It's devastating for those people who need those lifesaving services," King Young says. "People who need cancer treatment won't get it. Children with rheumatic heart disease won't get the heart surgeries that they need." All five of the U.S. territories affected — collectively home to more than 3 million Americans — are now desperately trying to figure out how to keep Medicaid running with only a fraction of the money they've had for the last several years. If Congress doesn't increase the amount of designated money by the end of the year, the U.S. Virgin Islands and Guam say they would need to cut their Medicaid rolls in half; Puerto Rico says it would need to cut back dental and prescription drug services. This is what people working on the issue have come to call the "Medicaid cliff." How did we get here?
When it comes to Medicaid, the federal government treats U.S. territories differently from how it treats states. But that's not how it works in the territories, where even though the populations are all low income, the federal government's match rate is set in statute at 55%. What this translates to is that for every dollar a U.S. territory spends on Medicaid, the federal government contributes $1.25. The other significant difference is that the federal contribution to Medicaid in the territories is capped, with a set allotment of federal funds every year. Federal spending on Medicaid in states is not. In recent months, Congress has passed continuing resolutions that have allowed the territories' Medicaid programs to keep limping along. But without legislation that appropriates more money, the territories' Medicaid programs all are in serious trouble. Opponents of the bill in the Senate say they worry that the billions of dollars that the territories are requesting could be misspent. Some senators have raised particular concerns about Puerto Rico. During a recent corruption probe, a Puerto Rican Medicaid official was arrested — that news emerged just a few days before a committee hearing on the territories' Medicaid bill in July. "So that didn't help," Rep. Darren Soto, D-Fla, says. Integrity provisions were added to the House bill, he says, specifically addressing concerns about Puerto Rico. "We do need to take it seriously and make sure that tax dollars are safeguarded," he says, but adds, "There have been fraud instances in many states too, and we don't take away their Medicaid funding." Some congressional Republicans note that the funding cliff was created by the Affordable Care Act, which gave extra funding to the territories for a limited time. In a letter to Secretary of Health and Human Services Alex Azar in July, several Republican members of the Senate Finance Committee raised concerns about Puerto Rico's Medicaid spending. "We are again confronting proposals for what amounts to another extension of boosted funding with no permanence or certainty and without any resolution of the Medicaid funding cliff constructed as part of the ACA," they wrote. "It is true: Giving these additional funds with a set expiration date, the legislation itself did create the cliff," acknowledges Robin Rudowitz, who co-directs the Program on Medicaid and the Uninsured at the Kaiser Family Foundation. However, she says, Congress now should consider "the implications of letting that cliff happen and what that means to the health care systems in these territories." - See the full NPR story. |